{"title":"改善癌症医院医生报告和记录严重警报的合规性。","authors":"Wania Imtiaz, Khawaja Shehryar Nasir, Fareeha Kanwal, Sheeba Saqib, Haroon Hafeez","doi":"10.37029/jcas.v7i2.419","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>A critical result of an investigation is considered a representation of a pathophysiological state deemed to be high risk or life threatening for the patient. Therefore, such results should be addressed in an appropriate and timely manner. Unfortunately, routine closed chart audits suggested that the compliance of physicians in documenting critical alerts in patient notes was poor. This prompted the hospital to conduct a continuous quality improvement (CQI) project to improve the physicians' compliance.</p><p><strong>Materials and methods: </strong>A cause-and-effect analysis was conducted using a fishbone diagram to identify the reasons for poor compliance. Based on the analysis, several modifications were made, including, but not limited to, hospital-wide educational sessions on the standard operating procedures of receiving and documenting critical alerts for the physicians, daily audit of critical alerts to review the appropriateness of documentation and introduction of a new module in the hospital electronic medical record to acknowledge and document receiving critical alerts.</p><p><strong>Results: </strong>Before implementing the strategies to improve physicians' documentation compliance, the average compliance rate was 57% in April 2020, and the median compliance rate was 52% (January 2020-April 2020). However, afterward, within a couple of months of implementing changes, the average compliance rate increased to 88%. This improvement was sustained for the next 8 months (median of 89%).</p><p><strong>Conclusion: </strong>This study found that CQI approach can be used to improve the compliance of the physicians for appropriately and timely documenting critical alerts, in this case, by continued education and training process and incorporating changes into the electronic hospital information system.</p>","PeriodicalId":73631,"journal":{"name":"Journal of cancer & allied specialties","volume":"7 2","pages":"e419"},"PeriodicalIF":0.0000,"publicationDate":"2021-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d2/c1/JCAS-7-419.PMC10166344.pdf","citationCount":"0","resultStr":"{\"title\":\"Improving Compliance of Physicians in Reporting and Documenting Critical Alerts in a Cancer Hospital.\",\"authors\":\"Wania Imtiaz, Khawaja Shehryar Nasir, Fareeha Kanwal, Sheeba Saqib, Haroon Hafeez\",\"doi\":\"10.37029/jcas.v7i2.419\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>A critical result of an investigation is considered a representation of a pathophysiological state deemed to be high risk or life threatening for the patient. Therefore, such results should be addressed in an appropriate and timely manner. Unfortunately, routine closed chart audits suggested that the compliance of physicians in documenting critical alerts in patient notes was poor. This prompted the hospital to conduct a continuous quality improvement (CQI) project to improve the physicians' compliance.</p><p><strong>Materials and methods: </strong>A cause-and-effect analysis was conducted using a fishbone diagram to identify the reasons for poor compliance. Based on the analysis, several modifications were made, including, but not limited to, hospital-wide educational sessions on the standard operating procedures of receiving and documenting critical alerts for the physicians, daily audit of critical alerts to review the appropriateness of documentation and introduction of a new module in the hospital electronic medical record to acknowledge and document receiving critical alerts.</p><p><strong>Results: </strong>Before implementing the strategies to improve physicians' documentation compliance, the average compliance rate was 57% in April 2020, and the median compliance rate was 52% (January 2020-April 2020). However, afterward, within a couple of months of implementing changes, the average compliance rate increased to 88%. This improvement was sustained for the next 8 months (median of 89%).</p><p><strong>Conclusion: </strong>This study found that CQI approach can be used to improve the compliance of the physicians for appropriately and timely documenting critical alerts, in this case, by continued education and training process and incorporating changes into the electronic hospital information system.</p>\",\"PeriodicalId\":73631,\"journal\":{\"name\":\"Journal of cancer & allied specialties\",\"volume\":\"7 2\",\"pages\":\"e419\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-05-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d2/c1/JCAS-7-419.PMC10166344.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of cancer & allied specialties\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.37029/jcas.v7i2.419\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cancer & allied specialties","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.37029/jcas.v7i2.419","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Improving Compliance of Physicians in Reporting and Documenting Critical Alerts in a Cancer Hospital.
Introduction: A critical result of an investigation is considered a representation of a pathophysiological state deemed to be high risk or life threatening for the patient. Therefore, such results should be addressed in an appropriate and timely manner. Unfortunately, routine closed chart audits suggested that the compliance of physicians in documenting critical alerts in patient notes was poor. This prompted the hospital to conduct a continuous quality improvement (CQI) project to improve the physicians' compliance.
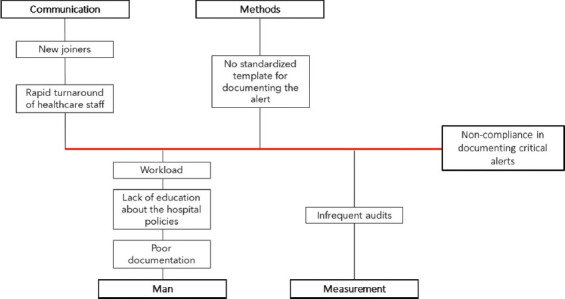
Materials and methods: A cause-and-effect analysis was conducted using a fishbone diagram to identify the reasons for poor compliance. Based on the analysis, several modifications were made, including, but not limited to, hospital-wide educational sessions on the standard operating procedures of receiving and documenting critical alerts for the physicians, daily audit of critical alerts to review the appropriateness of documentation and introduction of a new module in the hospital electronic medical record to acknowledge and document receiving critical alerts.
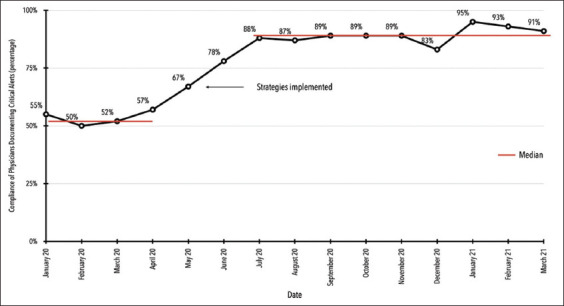
Results: Before implementing the strategies to improve physicians' documentation compliance, the average compliance rate was 57% in April 2020, and the median compliance rate was 52% (January 2020-April 2020). However, afterward, within a couple of months of implementing changes, the average compliance rate increased to 88%. This improvement was sustained for the next 8 months (median of 89%).
Conclusion: This study found that CQI approach can be used to improve the compliance of the physicians for appropriately and timely documenting critical alerts, in this case, by continued education and training process and incorporating changes into the electronic hospital information system.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
