Iain S Elliott, Conor Kleweno, Julie Agel, Max Coale, Joseph T Patterson, Reza Firoozabadi, Michael Githens, Niels V Johnsen
{"title":"髋臼骨折后勃起功能障碍。","authors":"Iain S Elliott, Conor Kleweno, Julie Agel, Max Coale, Joseph T Patterson, Reza Firoozabadi, Michael Githens, Niels V Johnsen","doi":"10.1097/OI9.0000000000000276","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To determine the rate of erectile dysfunction in male patients who have sustained an acetabular fracture with no previously identified urogenital injury.</p><p><strong>Design: </strong>Cross-sectional survey.</p><p><strong>Setting: </strong>Level 1 Trauma Center.</p><p><strong>Patients/participants: </strong>All male patients treated for acetabular fracture without urogenital injury.</p><p><strong>Intervention: </strong>The International Index of Erectile Function (IIEF), a validated patient-reported outcome measure for male sexual function, was administered to all patients.</p><p><strong>Main outcome measurements: </strong>Patients were asked to complete the International Index of Erectile Function score for both preinjury and current sexual function, and the erectile function (EF) domain was used to quantify the degree of erectile dysfunction. Fractures were classified according the OTA/AO classification schema, fracture classification, injury severity score, race, and treatment details, including surgical approach were collected from the database.</p><p><strong>Results: </strong>Ninety-two men with acetabular fractures without previously diagnosed urogenital injury responded to the survey at a minimum of 12 months and an average of 43 ± 21 months postinjury. The mean age was 53 ± 15 years. 39.8% of patients developed moderate-to-severe erectile dysfunction after injury. The mean EF domain score decreased 5.02 ± 1.73 points, which is greater than the minimum clinically important difference of 4. Increased injury severity score and associated fracture pattern were predictive of decreased EF score.</p><p><strong>Conclusion: </strong>Patients with acetabular fractures have an increased rate of erectile dysfunction at intermediate-term follow-up. The orthopaedic trauma surgeon treating these injuries should be aware of this as a potential associated injury, ask their patients about their function, and make appropriate referrals.</p><p><strong>Level of evidence: </strong>III.</p>","PeriodicalId":74381,"journal":{"name":"OTA international : the open access journal of orthopaedic trauma","volume":"6 2","pages":"e276"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d8/99/oi9-6-e276.PMC10194699.pdf","citationCount":"0","resultStr":"{\"title\":\"Erectile dysfunction after acetabular fracture.\",\"authors\":\"Iain S Elliott, Conor Kleweno, Julie Agel, Max Coale, Joseph T Patterson, Reza Firoozabadi, Michael Githens, Niels V Johnsen\",\"doi\":\"10.1097/OI9.0000000000000276\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To determine the rate of erectile dysfunction in male patients who have sustained an acetabular fracture with no previously identified urogenital injury.</p><p><strong>Design: </strong>Cross-sectional survey.</p><p><strong>Setting: </strong>Level 1 Trauma Center.</p><p><strong>Patients/participants: </strong>All male patients treated for acetabular fracture without urogenital injury.</p><p><strong>Intervention: </strong>The International Index of Erectile Function (IIEF), a validated patient-reported outcome measure for male sexual function, was administered to all patients.</p><p><strong>Main outcome measurements: </strong>Patients were asked to complete the International Index of Erectile Function score for both preinjury and current sexual function, and the erectile function (EF) domain was used to quantify the degree of erectile dysfunction. Fractures were classified according the OTA/AO classification schema, fracture classification, injury severity score, race, and treatment details, including surgical approach were collected from the database.</p><p><strong>Results: </strong>Ninety-two men with acetabular fractures without previously diagnosed urogenital injury responded to the survey at a minimum of 12 months and an average of 43 ± 21 months postinjury. The mean age was 53 ± 15 years. 39.8% of patients developed moderate-to-severe erectile dysfunction after injury. The mean EF domain score decreased 5.02 ± 1.73 points, which is greater than the minimum clinically important difference of 4. Increased injury severity score and associated fracture pattern were predictive of decreased EF score.</p><p><strong>Conclusion: </strong>Patients with acetabular fractures have an increased rate of erectile dysfunction at intermediate-term follow-up. The orthopaedic trauma surgeon treating these injuries should be aware of this as a potential associated injury, ask their patients about their function, and make appropriate referrals.</p><p><strong>Level of evidence: </strong>III.</p>\",\"PeriodicalId\":74381,\"journal\":{\"name\":\"OTA international : the open access journal of orthopaedic trauma\",\"volume\":\"6 2\",\"pages\":\"e276\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d8/99/oi9-6-e276.PMC10194699.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"OTA international : the open access journal of orthopaedic trauma\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/OI9.0000000000000276\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"OTA international : the open access journal of orthopaedic trauma","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/OI9.0000000000000276","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Objectives: To determine the rate of erectile dysfunction in male patients who have sustained an acetabular fracture with no previously identified urogenital injury.
Design: Cross-sectional survey.
Setting: Level 1 Trauma Center.
Patients/participants: All male patients treated for acetabular fracture without urogenital injury.
Intervention: The International Index of Erectile Function (IIEF), a validated patient-reported outcome measure for male sexual function, was administered to all patients.
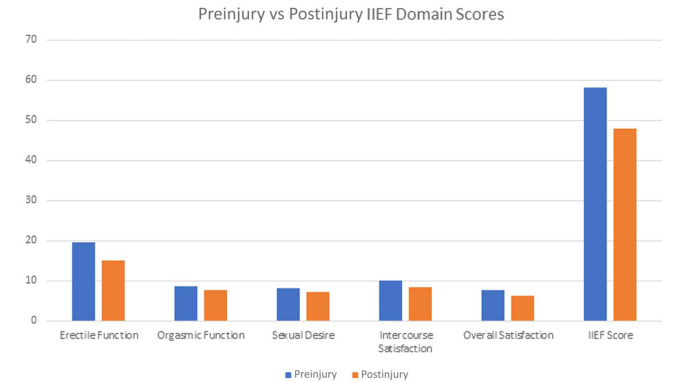
Main outcome measurements: Patients were asked to complete the International Index of Erectile Function score for both preinjury and current sexual function, and the erectile function (EF) domain was used to quantify the degree of erectile dysfunction. Fractures were classified according the OTA/AO classification schema, fracture classification, injury severity score, race, and treatment details, including surgical approach were collected from the database.
Results: Ninety-two men with acetabular fractures without previously diagnosed urogenital injury responded to the survey at a minimum of 12 months and an average of 43 ± 21 months postinjury. The mean age was 53 ± 15 years. 39.8% of patients developed moderate-to-severe erectile dysfunction after injury. The mean EF domain score decreased 5.02 ± 1.73 points, which is greater than the minimum clinically important difference of 4. Increased injury severity score and associated fracture pattern were predictive of decreased EF score.
Conclusion: Patients with acetabular fractures have an increased rate of erectile dysfunction at intermediate-term follow-up. The orthopaedic trauma surgeon treating these injuries should be aware of this as a potential associated injury, ask their patients about their function, and make appropriate referrals.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
