Shivani Shah, Ryan Sweeney, Maitreyee Rai, Deep Shah
{"title":"万古霉素致严重免疫性血小板减少症1例。","authors":"Shivani Shah, Ryan Sweeney, Maitreyee Rai, Deep Shah","doi":"10.3390/hematolrep15020028","DOIUrl":null,"url":null,"abstract":"<p><p>A male in his 60s presented with left lower extremity fractures following a vehicle accident. Hemoglobin, initially, was 12.4 mmol/L, and platelet count was 235 k/mcl. On day 11 of admission, his platelet count initially dropped to 99 k/mcl, and after recovery it rapidly decreased to 11 k/mcl on day 16 when the INR was 1.3 and aPTT was 32 s, and he continued to have a stable anemia throughout admission. There was no response in platelet count post-transfusion of four units of platelets. Hematology initially evaluated the patient for disseminated intravascular coagulation, heparin-induced thrombocytopenia (anti-PF4 antibody was 0.19), and thrombotic thrombocytopenic purpura (PLASMIC score of 4). Vancomycin was administered on days 1-7 for broad spectrum antimicrobial coverage and day 10, again, for concerns of sepsis. Given the temporal association of thrombocytopenia and vancomycin administration, a diagnosis of vancomycin-induced immune thrombocytopenia was established. Vancomycin was discontinued, and 2 doses of 1000 mg/kg of intravenous immunoglobulin 24 h apart were administered with the subsequent resolution of thrombocytopenia.</p>","PeriodicalId":12829,"journal":{"name":"Hematology Reports","volume":"15 2","pages":"283-289"},"PeriodicalIF":1.2000,"publicationDate":"2023-04-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10204526/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Case of Vancomycin-Induced Severe Immune Thrombocytopenia.\",\"authors\":\"Shivani Shah, Ryan Sweeney, Maitreyee Rai, Deep Shah\",\"doi\":\"10.3390/hematolrep15020028\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>A male in his 60s presented with left lower extremity fractures following a vehicle accident. Hemoglobin, initially, was 12.4 mmol/L, and platelet count was 235 k/mcl. On day 11 of admission, his platelet count initially dropped to 99 k/mcl, and after recovery it rapidly decreased to 11 k/mcl on day 16 when the INR was 1.3 and aPTT was 32 s, and he continued to have a stable anemia throughout admission. There was no response in platelet count post-transfusion of four units of platelets. Hematology initially evaluated the patient for disseminated intravascular coagulation, heparin-induced thrombocytopenia (anti-PF4 antibody was 0.19), and thrombotic thrombocytopenic purpura (PLASMIC score of 4). Vancomycin was administered on days 1-7 for broad spectrum antimicrobial coverage and day 10, again, for concerns of sepsis. Given the temporal association of thrombocytopenia and vancomycin administration, a diagnosis of vancomycin-induced immune thrombocytopenia was established. Vancomycin was discontinued, and 2 doses of 1000 mg/kg of intravenous immunoglobulin 24 h apart were administered with the subsequent resolution of thrombocytopenia.</p>\",\"PeriodicalId\":12829,\"journal\":{\"name\":\"Hematology Reports\",\"volume\":\"15 2\",\"pages\":\"283-289\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-04-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10204526/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hematology Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/hematolrep15020028\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hematology Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/hematolrep15020028","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
A Case of Vancomycin-Induced Severe Immune Thrombocytopenia.
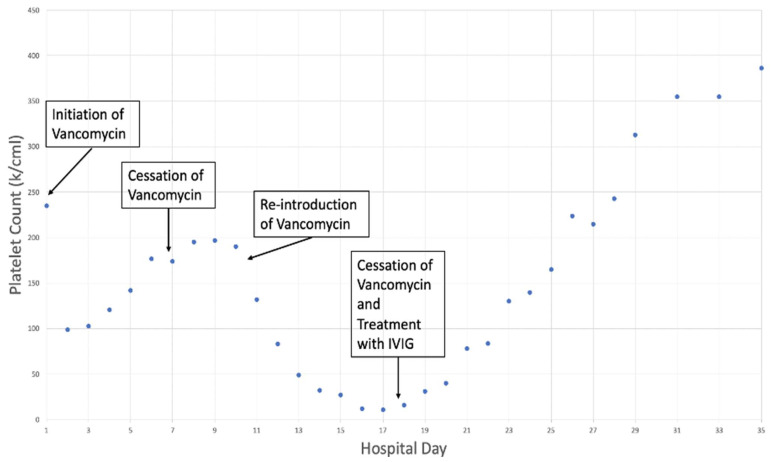
A male in his 60s presented with left lower extremity fractures following a vehicle accident. Hemoglobin, initially, was 12.4 mmol/L, and platelet count was 235 k/mcl. On day 11 of admission, his platelet count initially dropped to 99 k/mcl, and after recovery it rapidly decreased to 11 k/mcl on day 16 when the INR was 1.3 and aPTT was 32 s, and he continued to have a stable anemia throughout admission. There was no response in platelet count post-transfusion of four units of platelets. Hematology initially evaluated the patient for disseminated intravascular coagulation, heparin-induced thrombocytopenia (anti-PF4 antibody was 0.19), and thrombotic thrombocytopenic purpura (PLASMIC score of 4). Vancomycin was administered on days 1-7 for broad spectrum antimicrobial coverage and day 10, again, for concerns of sepsis. Given the temporal association of thrombocytopenia and vancomycin administration, a diagnosis of vancomycin-induced immune thrombocytopenia was established. Vancomycin was discontinued, and 2 doses of 1000 mg/kg of intravenous immunoglobulin 24 h apart were administered with the subsequent resolution of thrombocytopenia.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
