Mukaram Rana, Margit Niethammer, Christian Sellin, Hilmar Dörge, Holger Eggebrecht, Volker Schächinger
{"title":"在跨学科心脏中心接受经导管主动脉瓣植入术(TAVI)的患者住院结果的发展:489例连续病例的单中心经验","authors":"Mukaram Rana, Margit Niethammer, Christian Sellin, Hilmar Dörge, Holger Eggebrecht, Volker Schächinger","doi":"10.26502/fccm.92920309","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Transcatheter Aortic Valve Implantation (TAVI) has emerged over time, reflected in appropriate adjustments in the European Society of Cardiology (ESC) guidelines in 2007, 2012 and 2017.</p><p><strong>Objective: </strong>The aim of this study was to analyze in-hospital outcomes after TAVI in the development within a single heart center over a period of 10 years depending on adjustments in the guidelines, infrastructural and procedural determinants.</p><p><strong>Methods: </strong>489 consecutive patients who underwent TAVI from 2010 and 2019 at our center were analyzed retrospectively. Patients were divided into 3 groups of different treatment circumstances depending on guidelines adjustments and local infrastructural progress (group 1: 2010-2015 (n = 132), group 2: 2016-2017 (n = 155), group 3: 2018-2019 (n = 202). The primary endpoint was defined as all-cause in-hospital mortality. Secondary endpoints were selected according to the Valve Academic Research Consortium (VARC)-2 definitions. Multivariate logistic regression analysis was performed to determine predictors of in-hospital mortality. Statistical significance was assumed for p < 0.05.</p><p><strong>Results: </strong>489 patients (346 (70.8 %) transfemoral and 143 (29.2 %) transapical) underwent TAVI. Comparing periods (group 1 vs. 2 vs. 3) age (82.1 ± 6.2 vs. 82.5 ± 4.8 vs. 81.1 ± 5.1 years, p = 0.012) and EuroSCORE II (8.4 ± 6.0 vs. 5.8 ± 4.9 vs. 5.5 ± 5.0 %, p < 0.001) declined over time. Rates of in-hospital mortality decreased significantly (9.1 % vs. 5.8 % vs. 2.5 %, p = 0.029), especially with observed-to-expected mortality ratios indicating a disproportionate decline of in-hospital mortality (1.08 vs. 1.00 vs. 0.45). Furthermore, post-procedural complications, such as acute kidney injury stage 3 (10.6 % vs. 3.2 % vs. 4.5 %, p = 0.016) and bleeding complications (14.4 % vs. 11.6 % vs 7.9 %, p = 0.165) decreased from group 1 to 3. However, rates of permanent pacemaker implantations (7.6 % vs. 11.0 % vs. 22.8 %, p < 0.001) increased, associated with a switch towards self-expanding valves (0.0 % vs. 61.3 % vs. 76.7 %, p < 0.001). Length of hospitalization as well as stay at intensive care and intermediate care unit could be reduced significantly during the observation period. In multivariate analysis age (OR: 1.103; 95 % CI: 1.013 - 1.202; p = 0.025), creatinine level before TAVI (OR: 1.497; 95 % CI: 1.013 - 2.212; p = 0.043), atrial fibrillation (OR: 2.956; 95 % CI: 1.127 - 7.749; p = 0.028) and procedure duration (OR: 1.017; 95 % CI: 1.009 - 1.025; p < 0.001) could be identified as independent predictors of in-hospital mortality.</p><p><strong>Conclusion: </strong>This study identified age, creatinine level before TAVI, the presence of atrial fibrillation and procedure duration as independent predictors for in-hospital mortality. Although these predictors decreased during the observation period, the decline in hospital-mortality was disproportionate, which was indicated by an observed-to-expected mortality ratio of 0.45 for the last observation period. However, it can be assumed that apart from patient-related factors, there were further institutional, technical and procedural developments, which ran in parallel and affected in-hospital mortality rates after TAVI.</p>","PeriodicalId":72523,"journal":{"name":"Cardiology and cardiovascular medicine","volume":"7 2","pages":"52-68"},"PeriodicalIF":0.0000,"publicationDate":"2023-03-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10167775/pdf/","citationCount":"0","resultStr":"{\"title\":\"Development of In-Hospital Outcomes in Patients undergoing Transcatheter Aortic Valve Implantation (TAVI) at an Interdisciplinary Heart Center: A Single-Center Experience of 489 Consecutive Cases.\",\"authors\":\"Mukaram Rana, Margit Niethammer, Christian Sellin, Hilmar Dörge, Holger Eggebrecht, Volker Schächinger\",\"doi\":\"10.26502/fccm.92920309\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Transcatheter Aortic Valve Implantation (TAVI) has emerged over time, reflected in appropriate adjustments in the European Society of Cardiology (ESC) guidelines in 2007, 2012 and 2017.</p><p><strong>Objective: </strong>The aim of this study was to analyze in-hospital outcomes after TAVI in the development within a single heart center over a period of 10 years depending on adjustments in the guidelines, infrastructural and procedural determinants.</p><p><strong>Methods: </strong>489 consecutive patients who underwent TAVI from 2010 and 2019 at our center were analyzed retrospectively. Patients were divided into 3 groups of different treatment circumstances depending on guidelines adjustments and local infrastructural progress (group 1: 2010-2015 (n = 132), group 2: 2016-2017 (n = 155), group 3: 2018-2019 (n = 202). The primary endpoint was defined as all-cause in-hospital mortality. Secondary endpoints were selected according to the Valve Academic Research Consortium (VARC)-2 definitions. Multivariate logistic regression analysis was performed to determine predictors of in-hospital mortality. Statistical significance was assumed for p < 0.05.</p><p><strong>Results: </strong>489 patients (346 (70.8 %) transfemoral and 143 (29.2 %) transapical) underwent TAVI. Comparing periods (group 1 vs. 2 vs. 3) age (82.1 ± 6.2 vs. 82.5 ± 4.8 vs. 81.1 ± 5.1 years, p = 0.012) and EuroSCORE II (8.4 ± 6.0 vs. 5.8 ± 4.9 vs. 5.5 ± 5.0 %, p < 0.001) declined over time. Rates of in-hospital mortality decreased significantly (9.1 % vs. 5.8 % vs. 2.5 %, p = 0.029), especially with observed-to-expected mortality ratios indicating a disproportionate decline of in-hospital mortality (1.08 vs. 1.00 vs. 0.45). Furthermore, post-procedural complications, such as acute kidney injury stage 3 (10.6 % vs. 3.2 % vs. 4.5 %, p = 0.016) and bleeding complications (14.4 % vs. 11.6 % vs 7.9 %, p = 0.165) decreased from group 1 to 3. However, rates of permanent pacemaker implantations (7.6 % vs. 11.0 % vs. 22.8 %, p < 0.001) increased, associated with a switch towards self-expanding valves (0.0 % vs. 61.3 % vs. 76.7 %, p < 0.001). Length of hospitalization as well as stay at intensive care and intermediate care unit could be reduced significantly during the observation period. In multivariate analysis age (OR: 1.103; 95 % CI: 1.013 - 1.202; p = 0.025), creatinine level before TAVI (OR: 1.497; 95 % CI: 1.013 - 2.212; p = 0.043), atrial fibrillation (OR: 2.956; 95 % CI: 1.127 - 7.749; p = 0.028) and procedure duration (OR: 1.017; 95 % CI: 1.009 - 1.025; p < 0.001) could be identified as independent predictors of in-hospital mortality.</p><p><strong>Conclusion: </strong>This study identified age, creatinine level before TAVI, the presence of atrial fibrillation and procedure duration as independent predictors for in-hospital mortality. Although these predictors decreased during the observation period, the decline in hospital-mortality was disproportionate, which was indicated by an observed-to-expected mortality ratio of 0.45 for the last observation period. However, it can be assumed that apart from patient-related factors, there were further institutional, technical and procedural developments, which ran in parallel and affected in-hospital mortality rates after TAVI.</p>\",\"PeriodicalId\":72523,\"journal\":{\"name\":\"Cardiology and cardiovascular medicine\",\"volume\":\"7 2\",\"pages\":\"52-68\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-03-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10167775/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology and cardiovascular medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.26502/fccm.92920309\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology and cardiovascular medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.26502/fccm.92920309","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Development of In-Hospital Outcomes in Patients undergoing Transcatheter Aortic Valve Implantation (TAVI) at an Interdisciplinary Heart Center: A Single-Center Experience of 489 Consecutive Cases.
Background: Transcatheter Aortic Valve Implantation (TAVI) has emerged over time, reflected in appropriate adjustments in the European Society of Cardiology (ESC) guidelines in 2007, 2012 and 2017.
Objective: The aim of this study was to analyze in-hospital outcomes after TAVI in the development within a single heart center over a period of 10 years depending on adjustments in the guidelines, infrastructural and procedural determinants.
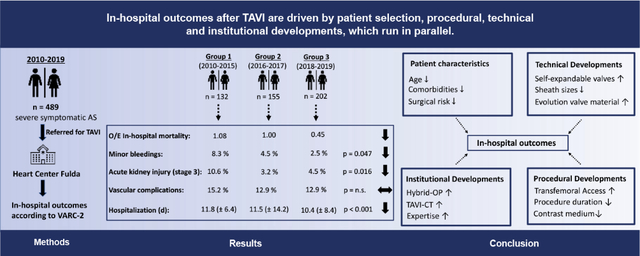
Methods: 489 consecutive patients who underwent TAVI from 2010 and 2019 at our center were analyzed retrospectively. Patients were divided into 3 groups of different treatment circumstances depending on guidelines adjustments and local infrastructural progress (group 1: 2010-2015 (n = 132), group 2: 2016-2017 (n = 155), group 3: 2018-2019 (n = 202). The primary endpoint was defined as all-cause in-hospital mortality. Secondary endpoints were selected according to the Valve Academic Research Consortium (VARC)-2 definitions. Multivariate logistic regression analysis was performed to determine predictors of in-hospital mortality. Statistical significance was assumed for p < 0.05.
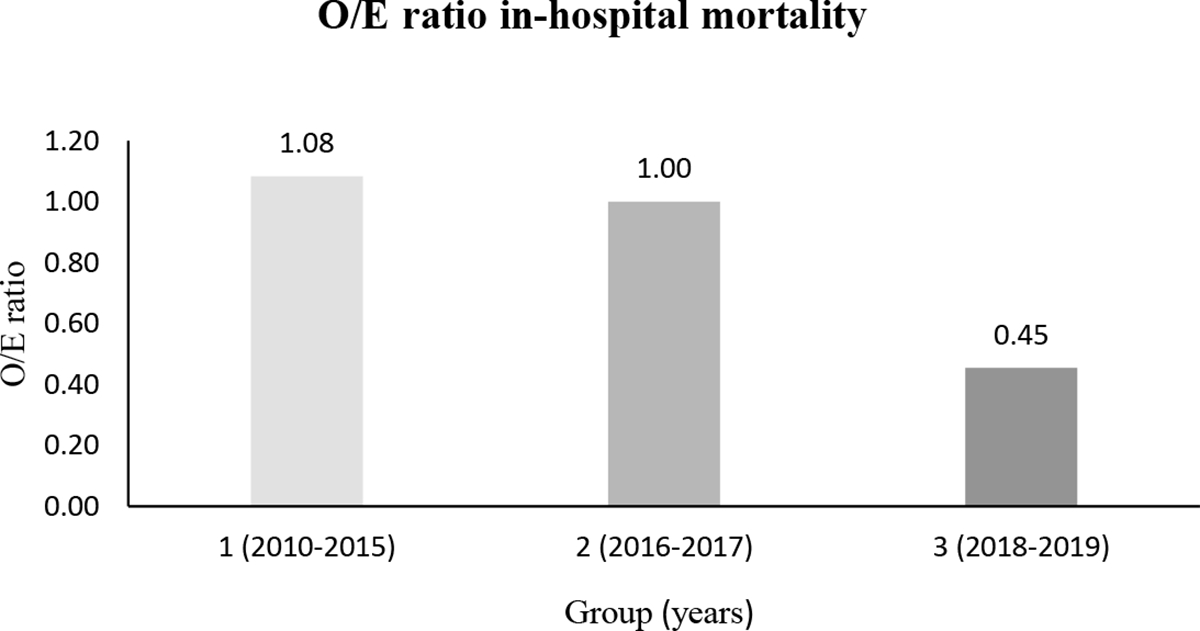
Results: 489 patients (346 (70.8 %) transfemoral and 143 (29.2 %) transapical) underwent TAVI. Comparing periods (group 1 vs. 2 vs. 3) age (82.1 ± 6.2 vs. 82.5 ± 4.8 vs. 81.1 ± 5.1 years, p = 0.012) and EuroSCORE II (8.4 ± 6.0 vs. 5.8 ± 4.9 vs. 5.5 ± 5.0 %, p < 0.001) declined over time. Rates of in-hospital mortality decreased significantly (9.1 % vs. 5.8 % vs. 2.5 %, p = 0.029), especially with observed-to-expected mortality ratios indicating a disproportionate decline of in-hospital mortality (1.08 vs. 1.00 vs. 0.45). Furthermore, post-procedural complications, such as acute kidney injury stage 3 (10.6 % vs. 3.2 % vs. 4.5 %, p = 0.016) and bleeding complications (14.4 % vs. 11.6 % vs 7.9 %, p = 0.165) decreased from group 1 to 3. However, rates of permanent pacemaker implantations (7.6 % vs. 11.0 % vs. 22.8 %, p < 0.001) increased, associated with a switch towards self-expanding valves (0.0 % vs. 61.3 % vs. 76.7 %, p < 0.001). Length of hospitalization as well as stay at intensive care and intermediate care unit could be reduced significantly during the observation period. In multivariate analysis age (OR: 1.103; 95 % CI: 1.013 - 1.202; p = 0.025), creatinine level before TAVI (OR: 1.497; 95 % CI: 1.013 - 2.212; p = 0.043), atrial fibrillation (OR: 2.956; 95 % CI: 1.127 - 7.749; p = 0.028) and procedure duration (OR: 1.017; 95 % CI: 1.009 - 1.025; p < 0.001) could be identified as independent predictors of in-hospital mortality.
Conclusion: This study identified age, creatinine level before TAVI, the presence of atrial fibrillation and procedure duration as independent predictors for in-hospital mortality. Although these predictors decreased during the observation period, the decline in hospital-mortality was disproportionate, which was indicated by an observed-to-expected mortality ratio of 0.45 for the last observation period. However, it can be assumed that apart from patient-related factors, there were further institutional, technical and procedural developments, which ran in parallel and affected in-hospital mortality rates after TAVI.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
