{"title":"修复或更换埃勒-丹洛斯综合征的二尖瓣?一个病例报告。","authors":"Raheleh Kavyani, Soheila Salari, Zeinab Norozi, Saeid Hosseini, Majid Maleki","doi":"10.18502/jthc.v18i1.12585","DOIUrl":null,"url":null,"abstract":"<p><p>Cardiac valvular Ehlers-Danlos syndrome (EDS) (type IV) is a rare subtype of the syndrome. The progressive and severe involvement of the heart valves is the principal characteristic of cardiovascular EDS, hence the necessity of the screening of patients with EDS for possible cardiovascular complications. We herein describe a 17-year-old male patient, with a known case of Ehlers-Danlos syndrome, who was referred to our center due to symptomatic severe mitral regurgitation. Echocardiography showed the flailing of the A3 scallop of the mitral valve (MV) and severe enlargement of the left ventricle and the left atrium with mild systolic dysfunction. A physical examination revealed joint hyperlaxity, skin hyperelasticity, and abdominal hernias. He was, therefore, scheduled for surgery. MV repair was performed via commissuroplasty and ring annuloplasty, with an acceptable saline test. After being weaned from cardiopulmonary bypass, the patient had mild mitral regurgitation, which escalated to moderate-to-severe mitral within minutes. Consequently, the MV was replaced with a bioprosthetic valve. The postoperative course was uneventful. Due to the high fragility of the MV, any resection and sewing of its fragile leaflets may produce residual regurgitation and necessitate valve replacement. MV replacement may be more logical in such patients. Our patient's postoperative course was uneventful, and he was discharged without symptoms. Over 1 and 3 months of follow-up, he remained asymptomatic, and transthoracic echocardiography showed a normal bioprosthetic MV without paravalvular leakage.</p>","PeriodicalId":39149,"journal":{"name":"Journal of Tehran University Heart Center","volume":"18 1","pages":"72-75"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bc/ed/JTHC-18-72.PMC10225027.pdf","citationCount":"0","resultStr":"{\"title\":\"To Repair or Replace the Mitral Valve in Ehlers-Danlos Syndrome? A Case Report.\",\"authors\":\"Raheleh Kavyani, Soheila Salari, Zeinab Norozi, Saeid Hosseini, Majid Maleki\",\"doi\":\"10.18502/jthc.v18i1.12585\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Cardiac valvular Ehlers-Danlos syndrome (EDS) (type IV) is a rare subtype of the syndrome. The progressive and severe involvement of the heart valves is the principal characteristic of cardiovascular EDS, hence the necessity of the screening of patients with EDS for possible cardiovascular complications. We herein describe a 17-year-old male patient, with a known case of Ehlers-Danlos syndrome, who was referred to our center due to symptomatic severe mitral regurgitation. Echocardiography showed the flailing of the A3 scallop of the mitral valve (MV) and severe enlargement of the left ventricle and the left atrium with mild systolic dysfunction. A physical examination revealed joint hyperlaxity, skin hyperelasticity, and abdominal hernias. He was, therefore, scheduled for surgery. MV repair was performed via commissuroplasty and ring annuloplasty, with an acceptable saline test. After being weaned from cardiopulmonary bypass, the patient had mild mitral regurgitation, which escalated to moderate-to-severe mitral within minutes. Consequently, the MV was replaced with a bioprosthetic valve. The postoperative course was uneventful. Due to the high fragility of the MV, any resection and sewing of its fragile leaflets may produce residual regurgitation and necessitate valve replacement. MV replacement may be more logical in such patients. Our patient's postoperative course was uneventful, and he was discharged without symptoms. Over 1 and 3 months of follow-up, he remained asymptomatic, and transthoracic echocardiography showed a normal bioprosthetic MV without paravalvular leakage.</p>\",\"PeriodicalId\":39149,\"journal\":{\"name\":\"Journal of Tehran University Heart Center\",\"volume\":\"18 1\",\"pages\":\"72-75\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bc/ed/JTHC-18-72.PMC10225027.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Tehran University Heart Center\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.18502/jthc.v18i1.12585\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Tehran University Heart Center","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18502/jthc.v18i1.12585","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
To Repair or Replace the Mitral Valve in Ehlers-Danlos Syndrome? A Case Report.
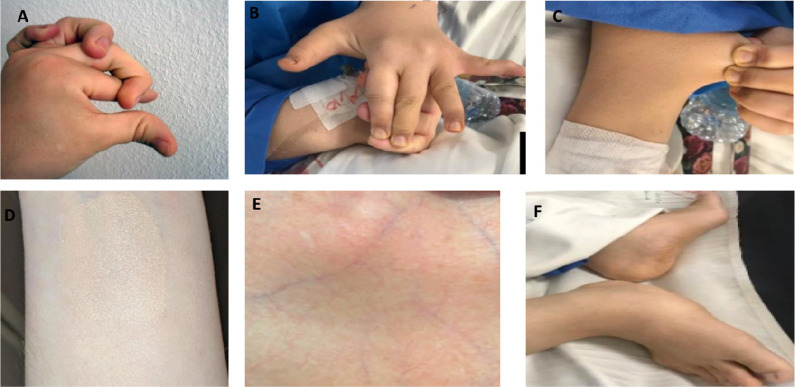
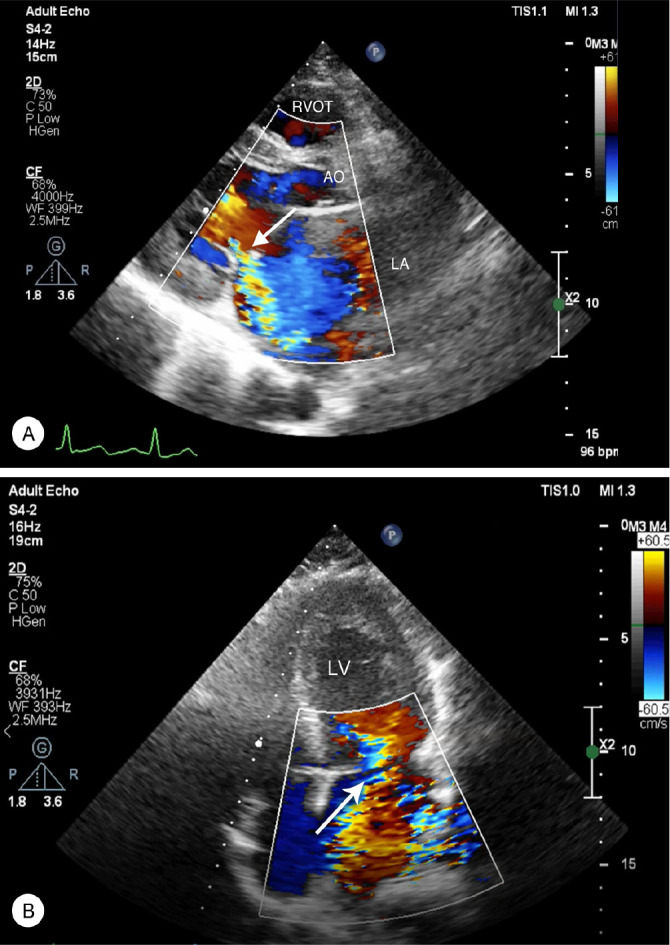
Cardiac valvular Ehlers-Danlos syndrome (EDS) (type IV) is a rare subtype of the syndrome. The progressive and severe involvement of the heart valves is the principal characteristic of cardiovascular EDS, hence the necessity of the screening of patients with EDS for possible cardiovascular complications. We herein describe a 17-year-old male patient, with a known case of Ehlers-Danlos syndrome, who was referred to our center due to symptomatic severe mitral regurgitation. Echocardiography showed the flailing of the A3 scallop of the mitral valve (MV) and severe enlargement of the left ventricle and the left atrium with mild systolic dysfunction. A physical examination revealed joint hyperlaxity, skin hyperelasticity, and abdominal hernias. He was, therefore, scheduled for surgery. MV repair was performed via commissuroplasty and ring annuloplasty, with an acceptable saline test. After being weaned from cardiopulmonary bypass, the patient had mild mitral regurgitation, which escalated to moderate-to-severe mitral within minutes. Consequently, the MV was replaced with a bioprosthetic valve. The postoperative course was uneventful. Due to the high fragility of the MV, any resection and sewing of its fragile leaflets may produce residual regurgitation and necessitate valve replacement. MV replacement may be more logical in such patients. Our patient's postoperative course was uneventful, and he was discharged without symptoms. Over 1 and 3 months of follow-up, he remained asymptomatic, and transthoracic echocardiography showed a normal bioprosthetic MV without paravalvular leakage.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
