{"title":"DeBakey血管扩张器在下肢重建中机械扩张受体血管2例报告。","authors":"Min-Gi Seo, Tae-Gon Kim","doi":"10.1055/s-0043-1764309","DOIUrl":null,"url":null,"abstract":"<p><p>In lower extremity reconstruction, the recipient vessel often requires long-range mechanical dilation because of extensive vasospasm or plaque formation induced by concomitant atherosclerosis. While a forceps dilator can be used to manipulate and dilate vessels approximately 1 cm from their end, a DeBakey vascular dilator can dilate long-range vessels. The authors successfully performed free flap reconstruction of the lower extremity using the DeBakey vascular dilator. Of the two patients who underwent lower extremity reconstruction, one had extensive vasospasm, and the other had plaques in the recipient arteries. Irrigation with 4% lidocaine and dilation of the lumen with a forceps dilator were insufficient to restore the normal arterial blood flow. Instead, a DeBakey vascular dilator with a 1-mm diameter tip was gently inserted into the lumen. Then, to overcome vessel resistance, the dilator gently advanced approximately 10 cm to dilate the recipient artery. Normal arterial blood flow was gushed out after dilating the vessel lumen using a DeBakey vascular dilator. The vascular anastomosis was performed, and intravenous heparin 5000 IU was administered immediately after anastomosis. Prophylactic low-molecular-weight-heparin (Clexane, 1 mg/kg) was administered subcutaneously to both patients for 14 days. The reconstructed flap survived without necrosis in either patient.</p>","PeriodicalId":47543,"journal":{"name":"Archives of Plastic Surgery-APS","volume":"50 3","pages":"311-314"},"PeriodicalIF":1.5000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10226792/pdf/","citationCount":"0","resultStr":"{\"title\":\"Mechanical Dilation of the Recipient Vessel with the DeBakey Vascular Dilator in Lower Extremity Reconstruction: A Report of Two Cases.\",\"authors\":\"Min-Gi Seo, Tae-Gon Kim\",\"doi\":\"10.1055/s-0043-1764309\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>In lower extremity reconstruction, the recipient vessel often requires long-range mechanical dilation because of extensive vasospasm or plaque formation induced by concomitant atherosclerosis. While a forceps dilator can be used to manipulate and dilate vessels approximately 1 cm from their end, a DeBakey vascular dilator can dilate long-range vessels. The authors successfully performed free flap reconstruction of the lower extremity using the DeBakey vascular dilator. Of the two patients who underwent lower extremity reconstruction, one had extensive vasospasm, and the other had plaques in the recipient arteries. Irrigation with 4% lidocaine and dilation of the lumen with a forceps dilator were insufficient to restore the normal arterial blood flow. Instead, a DeBakey vascular dilator with a 1-mm diameter tip was gently inserted into the lumen. Then, to overcome vessel resistance, the dilator gently advanced approximately 10 cm to dilate the recipient artery. Normal arterial blood flow was gushed out after dilating the vessel lumen using a DeBakey vascular dilator. The vascular anastomosis was performed, and intravenous heparin 5000 IU was administered immediately after anastomosis. Prophylactic low-molecular-weight-heparin (Clexane, 1 mg/kg) was administered subcutaneously to both patients for 14 days. The reconstructed flap survived without necrosis in either patient.</p>\",\"PeriodicalId\":47543,\"journal\":{\"name\":\"Archives of Plastic Surgery-APS\",\"volume\":\"50 3\",\"pages\":\"311-314\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10226792/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Archives of Plastic Surgery-APS\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0043-1764309\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Plastic Surgery-APS","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0043-1764309","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Mechanical Dilation of the Recipient Vessel with the DeBakey Vascular Dilator in Lower Extremity Reconstruction: A Report of Two Cases.
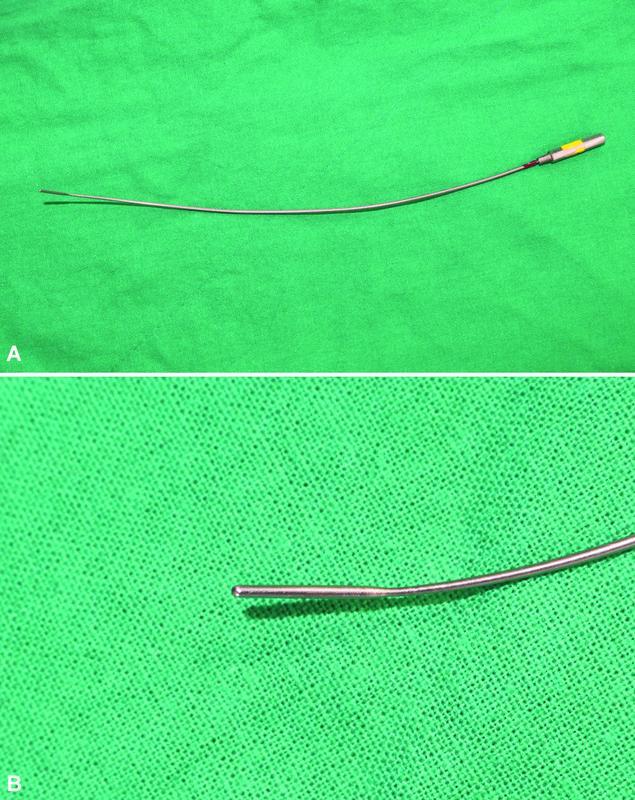
In lower extremity reconstruction, the recipient vessel often requires long-range mechanical dilation because of extensive vasospasm or plaque formation induced by concomitant atherosclerosis. While a forceps dilator can be used to manipulate and dilate vessels approximately 1 cm from their end, a DeBakey vascular dilator can dilate long-range vessels. The authors successfully performed free flap reconstruction of the lower extremity using the DeBakey vascular dilator. Of the two patients who underwent lower extremity reconstruction, one had extensive vasospasm, and the other had plaques in the recipient arteries. Irrigation with 4% lidocaine and dilation of the lumen with a forceps dilator were insufficient to restore the normal arterial blood flow. Instead, a DeBakey vascular dilator with a 1-mm diameter tip was gently inserted into the lumen. Then, to overcome vessel resistance, the dilator gently advanced approximately 10 cm to dilate the recipient artery. Normal arterial blood flow was gushed out after dilating the vessel lumen using a DeBakey vascular dilator. The vascular anastomosis was performed, and intravenous heparin 5000 IU was administered immediately after anastomosis. Prophylactic low-molecular-weight-heparin (Clexane, 1 mg/kg) was administered subcutaneously to both patients for 14 days. The reconstructed flap survived without necrosis in either patient.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
