Joseph M Zulu, Trevor Mwamba, Alyssa Rosen, Tulani Francis L Matenga, Joseph Mulanda, Mutale Kaimba, Masitano Chilembo, Madaliso Silondwa, Royd L Kamboyi, Sylvia Chila Simwanza, George Sichone, Malizgani Paul Chavula
{"title":"自愿医疗男性包皮环切术(VMMC)项目的社区参与:对赞比亚促进可持续项目的关键利益相关者角色的分析。","authors":"Joseph M Zulu, Trevor Mwamba, Alyssa Rosen, Tulani Francis L Matenga, Joseph Mulanda, Mutale Kaimba, Masitano Chilembo, Madaliso Silondwa, Royd L Kamboyi, Sylvia Chila Simwanza, George Sichone, Malizgani Paul Chavula","doi":"10.12688/gatesopenres.13587.2","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Within the Voluntary Medical Male Circumcision (VMMC) programme, community engagement has been central in facilitating the acceptance of VMMC, especially in non-circumcising communities. We used the case of the development of community engagement plans for sustainability of VMMC in Zambia to illustrate diversity of stakeholders, their power, roles, and strategies in community engagement. <b>Methods:</b> Data were collected using document review, in-depth interviews (n=35) and focus group discussions (n=35) with community stakeholders, health workers, health centre committees, counsellors, teachers, community volunteers and parents/caregivers. Data were analysed using thematic analysis. The analysis was guided by the power and interest model. <b>Results:</b> Differences were noted between the rural and urban sites in terms of power/influence and interest rating of community stakeholders who could be involved in the sustainability phase of the VMMC response in Zambia. For example, in the urban setting, neighbourhood health committees (NHCs), health workers, leaders of clubs, community health workers (CHWs), radio, television and social media platforms were ranked highest. From this list, social media and television platforms were not highly ranked in rural areas. Some stakeholders had more sources of power than others. Forms or sources of power included technical expertise, local authority, financial resources, collective action (action through schools, churches, media platforms, other community spaces), and relational power. Key roles and strategies included strengthening and broadening local coordination systems, enhancing community involvement, promoting community-led monitoring and evaluation, through the use of locally recognised communication spaces and channels, facilitating ownership of VMMC, and improving local accountability processes in VMMC activities. <b>Conclusions:</b> By consulting with the most relevant stakeholders, and considering community needs in programme development, the VMMC programme may be able to leverage the community structures and systems to reduce long term demand generation costs for VMMC and increase the acceptability and frequency of male circumcision.</p>","PeriodicalId":12593,"journal":{"name":"Gates Open Research","volume":"6 ","pages":"50"},"PeriodicalIF":0.0000,"publicationDate":"2023-05-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10105033/pdf/","citationCount":"0","resultStr":"{\"title\":\"Community engagement for the Voluntary Medical Male Circumcision (VMMC) program: an analysis of key stakeholder roles to promote a sustainable program in Zambia.\",\"authors\":\"Joseph M Zulu, Trevor Mwamba, Alyssa Rosen, Tulani Francis L Matenga, Joseph Mulanda, Mutale Kaimba, Masitano Chilembo, Madaliso Silondwa, Royd L Kamboyi, Sylvia Chila Simwanza, George Sichone, Malizgani Paul Chavula\",\"doi\":\"10.12688/gatesopenres.13587.2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Within the Voluntary Medical Male Circumcision (VMMC) programme, community engagement has been central in facilitating the acceptance of VMMC, especially in non-circumcising communities. We used the case of the development of community engagement plans for sustainability of VMMC in Zambia to illustrate diversity of stakeholders, their power, roles, and strategies in community engagement. <b>Methods:</b> Data were collected using document review, in-depth interviews (n=35) and focus group discussions (n=35) with community stakeholders, health workers, health centre committees, counsellors, teachers, community volunteers and parents/caregivers. Data were analysed using thematic analysis. The analysis was guided by the power and interest model. <b>Results:</b> Differences were noted between the rural and urban sites in terms of power/influence and interest rating of community stakeholders who could be involved in the sustainability phase of the VMMC response in Zambia. For example, in the urban setting, neighbourhood health committees (NHCs), health workers, leaders of clubs, community health workers (CHWs), radio, television and social media platforms were ranked highest. From this list, social media and television platforms were not highly ranked in rural areas. Some stakeholders had more sources of power than others. Forms or sources of power included technical expertise, local authority, financial resources, collective action (action through schools, churches, media platforms, other community spaces), and relational power. Key roles and strategies included strengthening and broadening local coordination systems, enhancing community involvement, promoting community-led monitoring and evaluation, through the use of locally recognised communication spaces and channels, facilitating ownership of VMMC, and improving local accountability processes in VMMC activities. <b>Conclusions:</b> By consulting with the most relevant stakeholders, and considering community needs in programme development, the VMMC programme may be able to leverage the community structures and systems to reduce long term demand generation costs for VMMC and increase the acceptability and frequency of male circumcision.</p>\",\"PeriodicalId\":12593,\"journal\":{\"name\":\"Gates Open Research\",\"volume\":\"6 \",\"pages\":\"50\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-05-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10105033/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gates Open Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12688/gatesopenres.13587.2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gates Open Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12688/gatesopenres.13587.2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Community engagement for the Voluntary Medical Male Circumcision (VMMC) program: an analysis of key stakeholder roles to promote a sustainable program in Zambia.
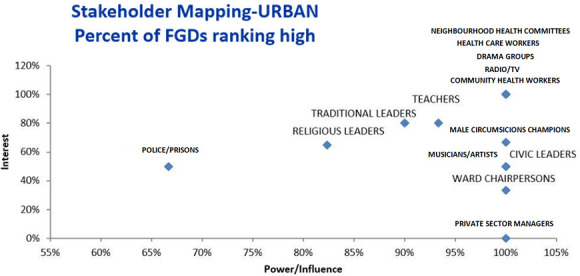
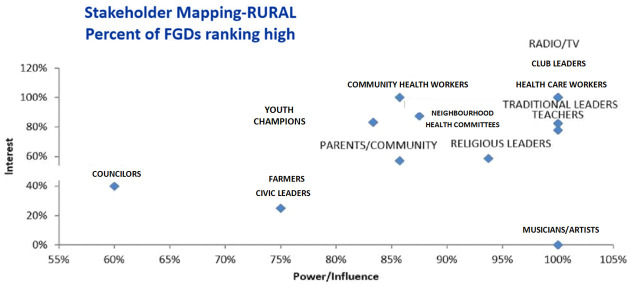
Background: Within the Voluntary Medical Male Circumcision (VMMC) programme, community engagement has been central in facilitating the acceptance of VMMC, especially in non-circumcising communities. We used the case of the development of community engagement plans for sustainability of VMMC in Zambia to illustrate diversity of stakeholders, their power, roles, and strategies in community engagement. Methods: Data were collected using document review, in-depth interviews (n=35) and focus group discussions (n=35) with community stakeholders, health workers, health centre committees, counsellors, teachers, community volunteers and parents/caregivers. Data were analysed using thematic analysis. The analysis was guided by the power and interest model. Results: Differences were noted between the rural and urban sites in terms of power/influence and interest rating of community stakeholders who could be involved in the sustainability phase of the VMMC response in Zambia. For example, in the urban setting, neighbourhood health committees (NHCs), health workers, leaders of clubs, community health workers (CHWs), radio, television and social media platforms were ranked highest. From this list, social media and television platforms were not highly ranked in rural areas. Some stakeholders had more sources of power than others. Forms or sources of power included technical expertise, local authority, financial resources, collective action (action through schools, churches, media platforms, other community spaces), and relational power. Key roles and strategies included strengthening and broadening local coordination systems, enhancing community involvement, promoting community-led monitoring and evaluation, through the use of locally recognised communication spaces and channels, facilitating ownership of VMMC, and improving local accountability processes in VMMC activities. Conclusions: By consulting with the most relevant stakeholders, and considering community needs in programme development, the VMMC programme may be able to leverage the community structures and systems to reduce long term demand generation costs for VMMC and increase the acceptability and frequency of male circumcision.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
