Pilar Mazón-Ramos, Sergio Cinza-Sanjurjo, David Garcia-Vega, Manuel Portela-Romero, Juan C Sanmartin-Pena, Daniel Rey-Aldana, Amparo Martinez-Monzonis, Jenifer Espasandín-Domínguez, Francisco Gude-Sampedro, José R González-Juanatey
{"title":"加利西亚医疗保健区心脏病科的临床医生对临床医生通用电子会诊计划提高了老年患者的医疗可及性和治疗效果。","authors":"Pilar Mazón-Ramos, Sergio Cinza-Sanjurjo, David Garcia-Vega, Manuel Portela-Romero, Juan C Sanmartin-Pena, Daniel Rey-Aldana, Amparo Martinez-Monzonis, Jenifer Espasandín-Domínguez, Francisco Gude-Sampedro, José R González-Juanatey","doi":"10.1093/ehjdh/ztad004","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>We aimed to assess longer-term results (accessibility, hospital admissions, and mortality) in elderly patients referred to a cardiology department (CD) from primary care using e-consultation in outpatient care.</p><p><strong>Methods and results: </strong>We included 9963 patients >80 years from 1 January 2010 to 31 December 2019. Until 2012, all patients attended an in-person consultation (2010-2012). In 2013, we instituted an e-consult programme (2013-2019) for all primary care referrals to cardiologists that preceded a patient's in-person consultation when considered. We used an interrupted time series (ITS) regression approach to investigate the impact of e-consultation on (i) cardiovascular hospital admissions and mortality. We also analysed (ii) the total number and referral rate (population-adjusted referred rate) in both periods, and (iii) the accessibility was measured as the number of consultations and variation according to the distance from the municipality and reference hospital. During e-consultation, the demand for care increased (12.8 ± 4.3% vs. 25.5 ± 11.1% per 1000 inhabitants, <i>P</i> < 0.001) and referrals from different areas were equalized. After the implementation of e-consultation, we observed that the increase in hospital admissions and mortality were stabilized [incidence rate ratio (iRR): 1.351 (95% CI, 0.787, 2.317), <i>P</i> = 0.874] and [iRR: 1.925 (95% CI: 0.889, 4.168), <i>P</i> = 0.096], respectively. The geographic variabilities in hospital admissions and mortality seen during the in-person consultation were stabilized after e-consultation implementation.</p><p><strong>Conclusions: </strong>Implementation of a clinician-to-clinician e-consultation programme in outpatient care was associated with improved accessibility to cardiology healthcare in elderly patients. After e-consultations were implemented, hospital admissions and mortality were stabilized.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"4 2","pages":"90-98"},"PeriodicalIF":4.4000,"publicationDate":"2023-01-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/73/1a/ztad004.PMC10039426.pdf","citationCount":"0","resultStr":"{\"title\":\"A clinician-to-clinician universal electronic consultation programme at the cardiology department of a Galician healthcare area improves healthcare accessibility and outcomes in elderly patients.\",\"authors\":\"Pilar Mazón-Ramos, Sergio Cinza-Sanjurjo, David Garcia-Vega, Manuel Portela-Romero, Juan C Sanmartin-Pena, Daniel Rey-Aldana, Amparo Martinez-Monzonis, Jenifer Espasandín-Domínguez, Francisco Gude-Sampedro, José R González-Juanatey\",\"doi\":\"10.1093/ehjdh/ztad004\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>We aimed to assess longer-term results (accessibility, hospital admissions, and mortality) in elderly patients referred to a cardiology department (CD) from primary care using e-consultation in outpatient care.</p><p><strong>Methods and results: </strong>We included 9963 patients >80 years from 1 January 2010 to 31 December 2019. Until 2012, all patients attended an in-person consultation (2010-2012). In 2013, we instituted an e-consult programme (2013-2019) for all primary care referrals to cardiologists that preceded a patient's in-person consultation when considered. We used an interrupted time series (ITS) regression approach to investigate the impact of e-consultation on (i) cardiovascular hospital admissions and mortality. We also analysed (ii) the total number and referral rate (population-adjusted referred rate) in both periods, and (iii) the accessibility was measured as the number of consultations and variation according to the distance from the municipality and reference hospital. During e-consultation, the demand for care increased (12.8 ± 4.3% vs. 25.5 ± 11.1% per 1000 inhabitants, <i>P</i> < 0.001) and referrals from different areas were equalized. After the implementation of e-consultation, we observed that the increase in hospital admissions and mortality were stabilized [incidence rate ratio (iRR): 1.351 (95% CI, 0.787, 2.317), <i>P</i> = 0.874] and [iRR: 1.925 (95% CI: 0.889, 4.168), <i>P</i> = 0.096], respectively. The geographic variabilities in hospital admissions and mortality seen during the in-person consultation were stabilized after e-consultation implementation.</p><p><strong>Conclusions: </strong>Implementation of a clinician-to-clinician e-consultation programme in outpatient care was associated with improved accessibility to cardiology healthcare in elderly patients. After e-consultations were implemented, hospital admissions and mortality were stabilized.</p>\",\"PeriodicalId\":72965,\"journal\":{\"name\":\"European heart journal. Digital health\",\"volume\":\"4 2\",\"pages\":\"90-98\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2023-01-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/73/1a/ztad004.PMC10039426.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal. Digital health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjdh/ztad004\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztad004","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/3/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
A clinician-to-clinician universal electronic consultation programme at the cardiology department of a Galician healthcare area improves healthcare accessibility and outcomes in elderly patients.
Aims: We aimed to assess longer-term results (accessibility, hospital admissions, and mortality) in elderly patients referred to a cardiology department (CD) from primary care using e-consultation in outpatient care.
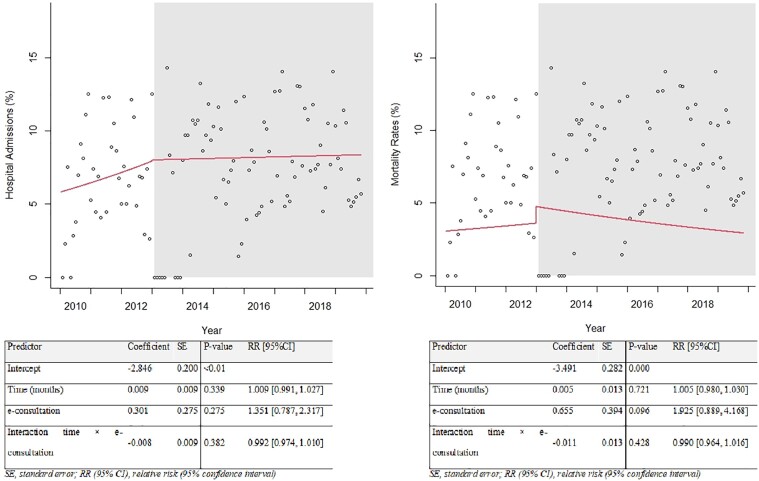
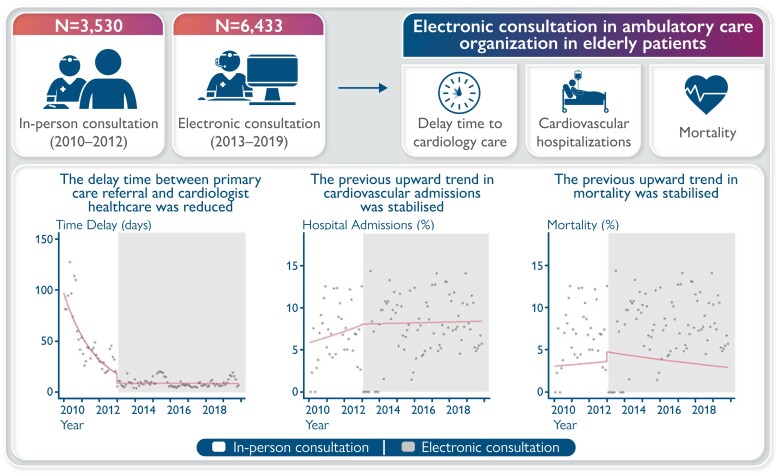
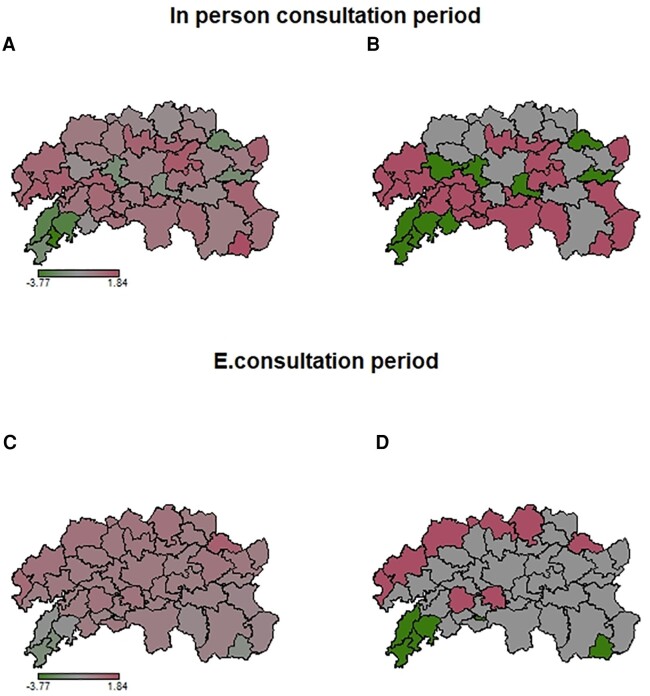
Methods and results: We included 9963 patients >80 years from 1 January 2010 to 31 December 2019. Until 2012, all patients attended an in-person consultation (2010-2012). In 2013, we instituted an e-consult programme (2013-2019) for all primary care referrals to cardiologists that preceded a patient's in-person consultation when considered. We used an interrupted time series (ITS) regression approach to investigate the impact of e-consultation on (i) cardiovascular hospital admissions and mortality. We also analysed (ii) the total number and referral rate (population-adjusted referred rate) in both periods, and (iii) the accessibility was measured as the number of consultations and variation according to the distance from the municipality and reference hospital. During e-consultation, the demand for care increased (12.8 ± 4.3% vs. 25.5 ± 11.1% per 1000 inhabitants, P < 0.001) and referrals from different areas were equalized. After the implementation of e-consultation, we observed that the increase in hospital admissions and mortality were stabilized [incidence rate ratio (iRR): 1.351 (95% CI, 0.787, 2.317), P = 0.874] and [iRR: 1.925 (95% CI: 0.889, 4.168), P = 0.096], respectively. The geographic variabilities in hospital admissions and mortality seen during the in-person consultation were stabilized after e-consultation implementation.
Conclusions: Implementation of a clinician-to-clinician e-consultation programme in outpatient care was associated with improved accessibility to cardiology healthcare in elderly patients. After e-consultations were implemented, hospital admissions and mortality were stabilized.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
