Jobbe Lemmens, Bastiaan Klarenbeek, Moniek Verstegen, Frans van Workum, Gerjon Hannink, Sander Ubels, Camiel Rosman
{"title":"基于共识的算法诊断癌症食管微创切除术后吻合口瘘的性能。","authors":"Jobbe Lemmens, Bastiaan Klarenbeek, Moniek Verstegen, Frans van Workum, Gerjon Hannink, Sander Ubels, Camiel Rosman","doi":"10.1093/dote/doad016","DOIUrl":null,"url":null,"abstract":"<p><p>Anastomotic leak (AL) is a common and severe complication after esophagectomy. This study aimed to assess the performance of a consensus-based algorithm for diagnosing AL after minimally invasive esophagectomy. This study used data of the ICAN trial, a multicenter randomized clinical trial comparing cervical and intrathoracic anastomosis, in which a predefined diagnostic algorithm was used to guide diagnosing AL. The algorithm identified patients suspected of AL based on clinical signs, blood C-reactive protein (cut-off value 200 mg/L), and/or drain amylase (cut-off value 200 IU/L). Suspicion of AL prompted evaluation with contrast swallow computed tomography and/or endoscopy to confirm AL. Primary outcome measure was algorithm performance in terms of sensitivity, specificity, and positive and negative predictive values (PPV, NPV), respectively. AL was defined according to the definition of the Esophagectomy Complications Consensus Group. 245 patients were included, and 125 (51%) patients were suspected of AL. The algorithm had a sensitivity of 62% (95% confidence interval [CI]: 46-75), a specificity of 97% (95% CI: 89-100), and a PPV and NPV of 94% (95% CI: 79-99) and 77% (95% CI: 66-86), respectively, on initial assessment. Repeated assessment in 19 patients with persisting suspicion of AL despite negative or inconclusive initial assessment had a sensitivity of 100% (95% CI: 77-100). The algorithm showed poor performance because the low sensitivity indicates the inability of the algorithm to confirm AL on initial assessment. Repeated assessment using the algorithm was needed to confirm remaining leaks.</p>","PeriodicalId":11255,"journal":{"name":"Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/62/ab/doad016.PMC10543373.pdf","citationCount":"0","resultStr":"{\"title\":\"Performance of a consensus-based algorithm for diagnosing anastomotic leak after minimally invasive esophagectomy for esophageal cancer.\",\"authors\":\"Jobbe Lemmens, Bastiaan Klarenbeek, Moniek Verstegen, Frans van Workum, Gerjon Hannink, Sander Ubels, Camiel Rosman\",\"doi\":\"10.1093/dote/doad016\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Anastomotic leak (AL) is a common and severe complication after esophagectomy. This study aimed to assess the performance of a consensus-based algorithm for diagnosing AL after minimally invasive esophagectomy. This study used data of the ICAN trial, a multicenter randomized clinical trial comparing cervical and intrathoracic anastomosis, in which a predefined diagnostic algorithm was used to guide diagnosing AL. The algorithm identified patients suspected of AL based on clinical signs, blood C-reactive protein (cut-off value 200 mg/L), and/or drain amylase (cut-off value 200 IU/L). Suspicion of AL prompted evaluation with contrast swallow computed tomography and/or endoscopy to confirm AL. Primary outcome measure was algorithm performance in terms of sensitivity, specificity, and positive and negative predictive values (PPV, NPV), respectively. AL was defined according to the definition of the Esophagectomy Complications Consensus Group. 245 patients were included, and 125 (51%) patients were suspected of AL. The algorithm had a sensitivity of 62% (95% confidence interval [CI]: 46-75), a specificity of 97% (95% CI: 89-100), and a PPV and NPV of 94% (95% CI: 79-99) and 77% (95% CI: 66-86), respectively, on initial assessment. Repeated assessment in 19 patients with persisting suspicion of AL despite negative or inconclusive initial assessment had a sensitivity of 100% (95% CI: 77-100). The algorithm showed poor performance because the low sensitivity indicates the inability of the algorithm to confirm AL on initial assessment. Repeated assessment using the algorithm was needed to confirm remaining leaks.</p>\",\"PeriodicalId\":11255,\"journal\":{\"name\":\"Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-09-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/62/ab/doad016.PMC10543373.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/dote/doad016\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/dote/doad016","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Performance of a consensus-based algorithm for diagnosing anastomotic leak after minimally invasive esophagectomy for esophageal cancer.
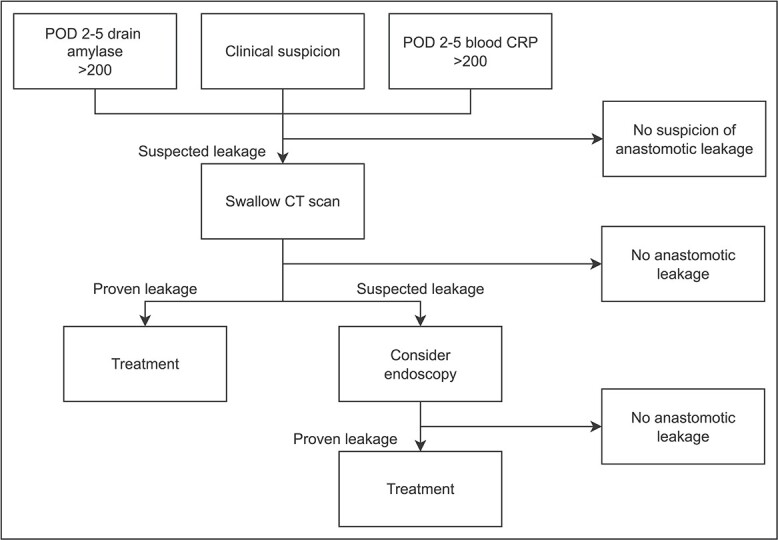
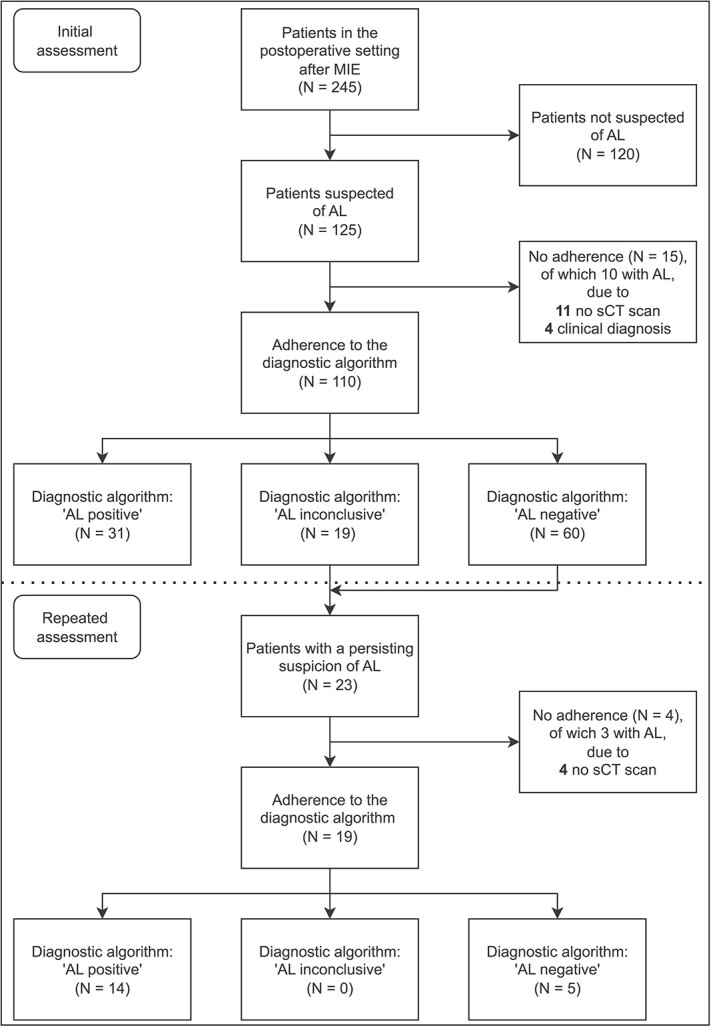
Anastomotic leak (AL) is a common and severe complication after esophagectomy. This study aimed to assess the performance of a consensus-based algorithm for diagnosing AL after minimally invasive esophagectomy. This study used data of the ICAN trial, a multicenter randomized clinical trial comparing cervical and intrathoracic anastomosis, in which a predefined diagnostic algorithm was used to guide diagnosing AL. The algorithm identified patients suspected of AL based on clinical signs, blood C-reactive protein (cut-off value 200 mg/L), and/or drain amylase (cut-off value 200 IU/L). Suspicion of AL prompted evaluation with contrast swallow computed tomography and/or endoscopy to confirm AL. Primary outcome measure was algorithm performance in terms of sensitivity, specificity, and positive and negative predictive values (PPV, NPV), respectively. AL was defined according to the definition of the Esophagectomy Complications Consensus Group. 245 patients were included, and 125 (51%) patients were suspected of AL. The algorithm had a sensitivity of 62% (95% confidence interval [CI]: 46-75), a specificity of 97% (95% CI: 89-100), and a PPV and NPV of 94% (95% CI: 79-99) and 77% (95% CI: 66-86), respectively, on initial assessment. Repeated assessment in 19 patients with persisting suspicion of AL despite negative or inconclusive initial assessment had a sensitivity of 100% (95% CI: 77-100). The algorithm showed poor performance because the low sensitivity indicates the inability of the algorithm to confirm AL on initial assessment. Repeated assessment using the algorithm was needed to confirm remaining leaks.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
