Shawnbir Gogia MD , Torsten P. Vahl MD , Vinod H. Thourani MD , Pradeep K. Yadav MD , Isaac George MD , Susheel K. Kodali MD , Nadira Hamid MD , Lauren Ranard MD , Tiffany Chen MD , Mitsuaki Matsumura BS , Akiko Maehara MD , Hendrik Treede MD, PhD , Stephan Baldus MD , David Daniels MD , Brett C. Sheridan MD , Firas Zahr MD , Mark J. Russo MD, MS , James M. McCabe MD , Stanley J. Chetcuti MD , Martin B. Leon MD , Omar K. Khalique MD
{"title":"针对原发性主动脉反流筛选专用经股导管瓣膜系统的患者的心脏计算机断层血管造影解剖特征","authors":"Shawnbir Gogia MD , Torsten P. Vahl MD , Vinod H. Thourani MD , Pradeep K. Yadav MD , Isaac George MD , Susheel K. Kodali MD , Nadira Hamid MD , Lauren Ranard MD , Tiffany Chen MD , Mitsuaki Matsumura BS , Akiko Maehara MD , Hendrik Treede MD, PhD , Stephan Baldus MD , David Daniels MD , Brett C. Sheridan MD , Firas Zahr MD , Mark J. Russo MD, MS , James M. McCabe MD , Stanley J. Chetcuti MD , Martin B. Leon MD , Omar K. Khalique MD","doi":"10.1016/j.shj.2023.100164","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Cardiac computed tomography angiography was used to identify anatomical characteristics of the aortic root in patients with severe aortic regurgitation (AR) as compared to those with aortic stenosis (AS) to judge feasibility of transcatheter aortic valve replacement (TAVR) with the JenaValve Trilogy system.</p></div><div><h3>Methods</h3><p>Cardiac computed tomography angiography was performed prior to planned TAVR for 107 patients with severe AR and 92 patients with severe AS. Measurements related to aortic root and coronary artery anatomy were obtained and compared between groups. Perimeter >90 mm and aortic annulus angle >70 degrees were defined as the theoretical exclusion criteria for TAVR. A combination of sinus of Valsalva diameter <30 mm and coronary height <12 mm was defined as high risk for coronary occlusion.</p></div><div><h3>Results</h3><p>The mean age of patients in the AR group was 74.9 ± 11.2 years, 46% were women, and the mean Society of Thoracic Surgeons risk score for mortality was 3.6 ± 2.1. Comparatively, the mean age of patients in the AS group was 82.3 ± 5.53 years, 65% were women, and the mean Society of Thoracic Surgeonsrisk score was 5.5 ± 3.3. Annulus area, perimeter, diameter, and angle were larger in patients with severe AR. Sinus of Valsalva diameters and heights were larger in patients with severe AR. More AR patients were excluded based on perimeter (14 vs. 2%) and annulus angle (6 vs. 1%). More AS patients exhibited high-risk anatomy for left main coronary occlusion (21 vs. 7%) and right coronary occlusion (14 vs. 3%). The maximum dimension of the ascending aorta was larger in patients with severe AR (39 vs. 35 mm). The percentage of referred AR patients with significant aortopathy requiring surgical intervention was very low (only 1 AR patient with ascending aorta diameter >5.5 cm).</p></div><div><h3>Conclusions</h3><p>A significantly larger proportion of patients with severe AR are excluded from TAVR as compared to AS due to large aortic annulus size and steep annulus angulation. By far the most prevalent excluding factor is aortic annulus size, with fewer patients excluded due to angulation. AR patients have lower-risk anatomy for coronary occlusion. Larger transcatheter valve sizes and further delivery system modifications are required to treat a larger proportion of AR patients.</p></div>","PeriodicalId":36053,"journal":{"name":"Structural Heart","volume":"7 3","pages":"Article 100164"},"PeriodicalIF":2.8000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10236804/pdf/","citationCount":"1","resultStr":"{\"title\":\"Cardiac Computed Tomography Angiography Anatomical Characterization of Patients Screened for a Dedicated Transfemoral Transcatheter Valve System for Primary Aortic Regurgitation\",\"authors\":\"Shawnbir Gogia MD , Torsten P. Vahl MD , Vinod H. Thourani MD , Pradeep K. Yadav MD , Isaac George MD , Susheel K. Kodali MD , Nadira Hamid MD , Lauren Ranard MD , Tiffany Chen MD , Mitsuaki Matsumura BS , Akiko Maehara MD , Hendrik Treede MD, PhD , Stephan Baldus MD , David Daniels MD , Brett C. Sheridan MD , Firas Zahr MD , Mark J. Russo MD, MS , James M. McCabe MD , Stanley J. Chetcuti MD , Martin B. Leon MD , Omar K. Khalique MD\",\"doi\":\"10.1016/j.shj.2023.100164\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Cardiac computed tomography angiography was used to identify anatomical characteristics of the aortic root in patients with severe aortic regurgitation (AR) as compared to those with aortic stenosis (AS) to judge feasibility of transcatheter aortic valve replacement (TAVR) with the JenaValve Trilogy system.</p></div><div><h3>Methods</h3><p>Cardiac computed tomography angiography was performed prior to planned TAVR for 107 patients with severe AR and 92 patients with severe AS. Measurements related to aortic root and coronary artery anatomy were obtained and compared between groups. Perimeter >90 mm and aortic annulus angle >70 degrees were defined as the theoretical exclusion criteria for TAVR. A combination of sinus of Valsalva diameter <30 mm and coronary height <12 mm was defined as high risk for coronary occlusion.</p></div><div><h3>Results</h3><p>The mean age of patients in the AR group was 74.9 ± 11.2 years, 46% were women, and the mean Society of Thoracic Surgeons risk score for mortality was 3.6 ± 2.1. Comparatively, the mean age of patients in the AS group was 82.3 ± 5.53 years, 65% were women, and the mean Society of Thoracic Surgeonsrisk score was 5.5 ± 3.3. Annulus area, perimeter, diameter, and angle were larger in patients with severe AR. Sinus of Valsalva diameters and heights were larger in patients with severe AR. More AR patients were excluded based on perimeter (14 vs. 2%) and annulus angle (6 vs. 1%). More AS patients exhibited high-risk anatomy for left main coronary occlusion (21 vs. 7%) and right coronary occlusion (14 vs. 3%). The maximum dimension of the ascending aorta was larger in patients with severe AR (39 vs. 35 mm). The percentage of referred AR patients with significant aortopathy requiring surgical intervention was very low (only 1 AR patient with ascending aorta diameter >5.5 cm).</p></div><div><h3>Conclusions</h3><p>A significantly larger proportion of patients with severe AR are excluded from TAVR as compared to AS due to large aortic annulus size and steep annulus angulation. By far the most prevalent excluding factor is aortic annulus size, with fewer patients excluded due to angulation. AR patients have lower-risk anatomy for coronary occlusion. Larger transcatheter valve sizes and further delivery system modifications are required to treat a larger proportion of AR patients.</p></div>\",\"PeriodicalId\":36053,\"journal\":{\"name\":\"Structural Heart\",\"volume\":\"7 3\",\"pages\":\"Article 100164\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2023-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10236804/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Structural Heart\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2474870623000118\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Structural Heart","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2474870623000118","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Cardiac Computed Tomography Angiography Anatomical Characterization of Patients Screened for a Dedicated Transfemoral Transcatheter Valve System for Primary Aortic Regurgitation
Background
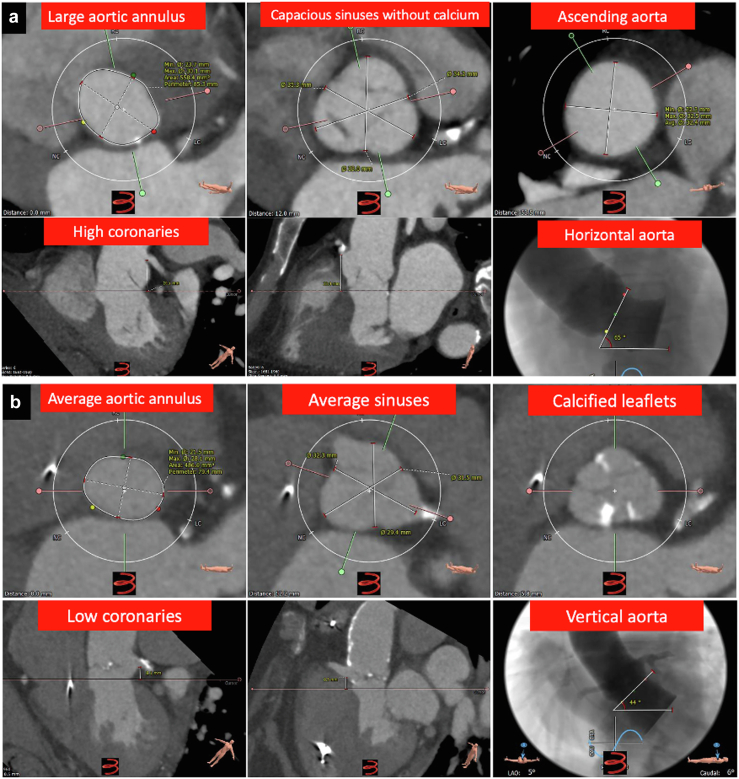
Cardiac computed tomography angiography was used to identify anatomical characteristics of the aortic root in patients with severe aortic regurgitation (AR) as compared to those with aortic stenosis (AS) to judge feasibility of transcatheter aortic valve replacement (TAVR) with the JenaValve Trilogy system.
Methods
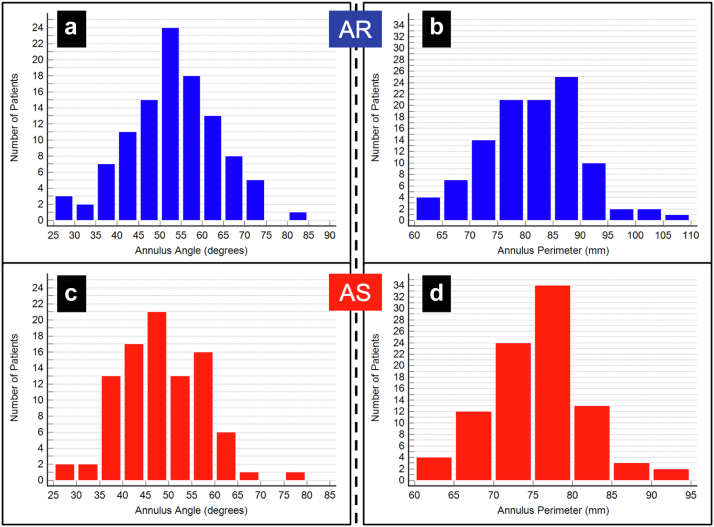
Cardiac computed tomography angiography was performed prior to planned TAVR for 107 patients with severe AR and 92 patients with severe AS. Measurements related to aortic root and coronary artery anatomy were obtained and compared between groups. Perimeter >90 mm and aortic annulus angle >70 degrees were defined as the theoretical exclusion criteria for TAVR. A combination of sinus of Valsalva diameter <30 mm and coronary height <12 mm was defined as high risk for coronary occlusion.
Results
The mean age of patients in the AR group was 74.9 ± 11.2 years, 46% were women, and the mean Society of Thoracic Surgeons risk score for mortality was 3.6 ± 2.1. Comparatively, the mean age of patients in the AS group was 82.3 ± 5.53 years, 65% were women, and the mean Society of Thoracic Surgeonsrisk score was 5.5 ± 3.3. Annulus area, perimeter, diameter, and angle were larger in patients with severe AR. Sinus of Valsalva diameters and heights were larger in patients with severe AR. More AR patients were excluded based on perimeter (14 vs. 2%) and annulus angle (6 vs. 1%). More AS patients exhibited high-risk anatomy for left main coronary occlusion (21 vs. 7%) and right coronary occlusion (14 vs. 3%). The maximum dimension of the ascending aorta was larger in patients with severe AR (39 vs. 35 mm). The percentage of referred AR patients with significant aortopathy requiring surgical intervention was very low (only 1 AR patient with ascending aorta diameter >5.5 cm).
Conclusions
A significantly larger proportion of patients with severe AR are excluded from TAVR as compared to AS due to large aortic annulus size and steep annulus angulation. By far the most prevalent excluding factor is aortic annulus size, with fewer patients excluded due to angulation. AR patients have lower-risk anatomy for coronary occlusion. Larger transcatheter valve sizes and further delivery system modifications are required to treat a larger proportion of AR patients.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
