Carolina Teles, Chiranthi Kongala Liyanage, Geoffrey Chow, Christopher P Denton, Voon Ong
{"title":"系统性硬化症复发性多软骨炎:一种罕见的血管样病变。","authors":"Carolina Teles, Chiranthi Kongala Liyanage, Geoffrey Chow, Christopher P Denton, Voon Ong","doi":"10.1177/23971983221141599","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Relapsing polychondritis is a rare, immune-mediated disease characterised by inflammation of cartilaginous structures. Auricular chondritis, sparing the fatty lobule, is the most typical feature, followed by nose and laryngotracheal involvement. Albeit rare, neurologic involvement is reported with relapsing polychondritis. Cranial nerve involvement is the most frequent neurologic manifestation and is probably due to an underlying vasculitic process. Approximately one-third of relapsing polychondritis patients can overlap with other systemic diseases, including other autoimmune connective tissue diseases, but association with systemic sclerosis has very rarely been described.</p><p><strong>Case description: </strong>A 63-year-old woman presented with acute new-onset severe dysphagia, accompanied by hoarseness and preceded by pain, swelling and erythema of the left pinna, unresponsive to antibiotics. She had a history of long-standing limited cutaneous systemic sclerosis. Cranial nerve examination revealed right-sided palatal palsy, and left vocal cord palsy was found on fibreoptic nasendoscopy. Magnetic resonance imaging of the head and neck showed bilateral enhancement of an extracranial segment of the glossopharyngeal and vagus nerves. Clinical features and imaging findings were consistent with relapsing polychondritis, which successfully responded to high-dose steroids.</p><p><strong>Conclusions: </strong>This is a case of relapsing polychondritis mimicking progression of systemic sclerosis, showcasing its challenging features. It emphasises the importance of early diagnosis and prompt management with potential impact on the outcome, while highlighting the complex interplay between these two disease entities and vasculitic mechanisms, which may reflect the shared network of genetic predisposition across autoimmune rheumatic diseases.</p>","PeriodicalId":17036,"journal":{"name":"Journal of Scleroderma and Related Disorders","volume":"8 2","pages":"NP4-NP8"},"PeriodicalIF":1.2000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10242694/pdf/","citationCount":"0","resultStr":"{\"title\":\"Relapsing polychondritis in systemic sclerosis: A rare vasculitic mimic.\",\"authors\":\"Carolina Teles, Chiranthi Kongala Liyanage, Geoffrey Chow, Christopher P Denton, Voon Ong\",\"doi\":\"10.1177/23971983221141599\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Relapsing polychondritis is a rare, immune-mediated disease characterised by inflammation of cartilaginous structures. Auricular chondritis, sparing the fatty lobule, is the most typical feature, followed by nose and laryngotracheal involvement. Albeit rare, neurologic involvement is reported with relapsing polychondritis. Cranial nerve involvement is the most frequent neurologic manifestation and is probably due to an underlying vasculitic process. Approximately one-third of relapsing polychondritis patients can overlap with other systemic diseases, including other autoimmune connective tissue diseases, but association with systemic sclerosis has very rarely been described.</p><p><strong>Case description: </strong>A 63-year-old woman presented with acute new-onset severe dysphagia, accompanied by hoarseness and preceded by pain, swelling and erythema of the left pinna, unresponsive to antibiotics. She had a history of long-standing limited cutaneous systemic sclerosis. Cranial nerve examination revealed right-sided palatal palsy, and left vocal cord palsy was found on fibreoptic nasendoscopy. Magnetic resonance imaging of the head and neck showed bilateral enhancement of an extracranial segment of the glossopharyngeal and vagus nerves. Clinical features and imaging findings were consistent with relapsing polychondritis, which successfully responded to high-dose steroids.</p><p><strong>Conclusions: </strong>This is a case of relapsing polychondritis mimicking progression of systemic sclerosis, showcasing its challenging features. It emphasises the importance of early diagnosis and prompt management with potential impact on the outcome, while highlighting the complex interplay between these two disease entities and vasculitic mechanisms, which may reflect the shared network of genetic predisposition across autoimmune rheumatic diseases.</p>\",\"PeriodicalId\":17036,\"journal\":{\"name\":\"Journal of Scleroderma and Related Disorders\",\"volume\":\"8 2\",\"pages\":\"NP4-NP8\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10242694/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Scleroderma and Related Disorders\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/23971983221141599\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Scleroderma and Related Disorders","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23971983221141599","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Relapsing polychondritis in systemic sclerosis: A rare vasculitic mimic.
Introduction: Relapsing polychondritis is a rare, immune-mediated disease characterised by inflammation of cartilaginous structures. Auricular chondritis, sparing the fatty lobule, is the most typical feature, followed by nose and laryngotracheal involvement. Albeit rare, neurologic involvement is reported with relapsing polychondritis. Cranial nerve involvement is the most frequent neurologic manifestation and is probably due to an underlying vasculitic process. Approximately one-third of relapsing polychondritis patients can overlap with other systemic diseases, including other autoimmune connective tissue diseases, but association with systemic sclerosis has very rarely been described.
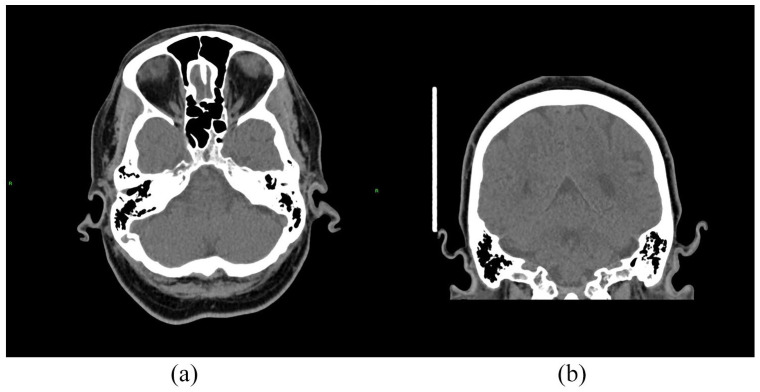
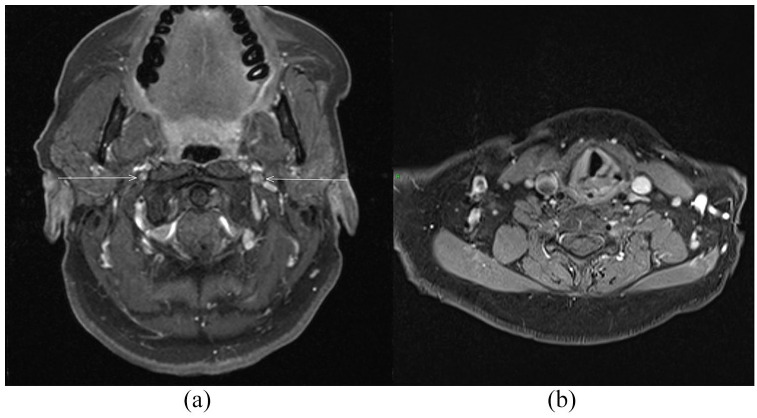
Case description: A 63-year-old woman presented with acute new-onset severe dysphagia, accompanied by hoarseness and preceded by pain, swelling and erythema of the left pinna, unresponsive to antibiotics. She had a history of long-standing limited cutaneous systemic sclerosis. Cranial nerve examination revealed right-sided palatal palsy, and left vocal cord palsy was found on fibreoptic nasendoscopy. Magnetic resonance imaging of the head and neck showed bilateral enhancement of an extracranial segment of the glossopharyngeal and vagus nerves. Clinical features and imaging findings were consistent with relapsing polychondritis, which successfully responded to high-dose steroids.
Conclusions: This is a case of relapsing polychondritis mimicking progression of systemic sclerosis, showcasing its challenging features. It emphasises the importance of early diagnosis and prompt management with potential impact on the outcome, while highlighting the complex interplay between these two disease entities and vasculitic mechanisms, which may reflect the shared network of genetic predisposition across autoimmune rheumatic diseases.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
