{"title":"一项回顾性观察研究:使用计算机断层扫描评估胃位置与危重患者幽门后肠内喂养管置入成功相关。","authors":"Masashi Yokose, Shunsuke Takaki, Yusuke Saigusa, Takahiro Mihara, Yoshinobu Ishiwata, Shingo Kato, Keiichi Horie, Takahisa Goto","doi":"10.1186/s40560-023-00673-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Post-pyloric enteral feeding reduces respiratory complications and shortens the duration of mechanical ventilation. Blind placement of post-pyloric enteral feeding tubes (EFT) in patients with critical illnesses is often the first-line method because endoscopy or fluoroscopy cannot be easily performed at bedside; however, difficult placements regularly occur. We reported an association between the stomach position caudal to spinal level L1-L2, evaluated by abdominal radiographs after placement, and difficult placement; however, this method could not indicate difficulty before EFT placement. The aim of our study was to evaluate the association between stomach position, estimated using computed tomography (CT) images taken before the blind placement of the post-pyloric EFT, and the difficulty of EFT placement.</p><p><strong>Methods: </strong>Data from patients aged ≥ 20 years who underwent post-pyloric EFT in our intensive care unit were obtained retrospectively. Logistic regression analysis was used to evaluate the association between successful initial EFT placement and explanatory variables, including stomach position estimated by CT. Two cut-off values were used: caudal to L1-L2 based on a previous study and the best cut-off value calculated by the receiver operating characteristic curve. Variable selection was performed backward stepwise using Akaike's Information Criterion.</p><p><strong>Results: </strong>Of the total of 453 patients who were enrolled, the success rate of the initial EFT placement was 43.5%. The adjusted odds ratio for successful initial EFT placement of the stomach position caudal to L1-L2 was 0.61 (95% confidence interval: 0.41-1.07). Logistic regression analysis, including the stomach position caudal to L2-L3, calculated as the best cut-off value, indicated that stomach position was an independent factor for failure of initial EFT placement (adjusted odds ratio, 0.55; 95% confidence interval: 0.33-0.91).</p><p><strong>Conclusions: </strong>Stomach position evaluated using CT images was associated with successful initial post-pyloric EFT placement. The best cut-off value of the greater curvature of the stomach to predict the success or failure of the first attempt was spinal level L2-L3. Trial registration University Hospital Medical Information Network Clinical Trials Registry (UMIN000046986; February 28, 2022). https://center6.umin.ac.jp/cgi-open-bin/ctr/ctr_view.cgi?recptno=R000052151.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"11 1","pages":"25"},"PeriodicalIF":4.7000,"publicationDate":"2023-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10228095/pdf/","citationCount":"0","resultStr":"{\"title\":\"Stomach position evaluated using computed tomography is related to successful post-pyloric enteral feeding tube placement in critically ill patients: a retrospective observational study.\",\"authors\":\"Masashi Yokose, Shunsuke Takaki, Yusuke Saigusa, Takahiro Mihara, Yoshinobu Ishiwata, Shingo Kato, Keiichi Horie, Takahisa Goto\",\"doi\":\"10.1186/s40560-023-00673-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Post-pyloric enteral feeding reduces respiratory complications and shortens the duration of mechanical ventilation. Blind placement of post-pyloric enteral feeding tubes (EFT) in patients with critical illnesses is often the first-line method because endoscopy or fluoroscopy cannot be easily performed at bedside; however, difficult placements regularly occur. We reported an association between the stomach position caudal to spinal level L1-L2, evaluated by abdominal radiographs after placement, and difficult placement; however, this method could not indicate difficulty before EFT placement. The aim of our study was to evaluate the association between stomach position, estimated using computed tomography (CT) images taken before the blind placement of the post-pyloric EFT, and the difficulty of EFT placement.</p><p><strong>Methods: </strong>Data from patients aged ≥ 20 years who underwent post-pyloric EFT in our intensive care unit were obtained retrospectively. Logistic regression analysis was used to evaluate the association between successful initial EFT placement and explanatory variables, including stomach position estimated by CT. Two cut-off values were used: caudal to L1-L2 based on a previous study and the best cut-off value calculated by the receiver operating characteristic curve. Variable selection was performed backward stepwise using Akaike's Information Criterion.</p><p><strong>Results: </strong>Of the total of 453 patients who were enrolled, the success rate of the initial EFT placement was 43.5%. The adjusted odds ratio for successful initial EFT placement of the stomach position caudal to L1-L2 was 0.61 (95% confidence interval: 0.41-1.07). Logistic regression analysis, including the stomach position caudal to L2-L3, calculated as the best cut-off value, indicated that stomach position was an independent factor for failure of initial EFT placement (adjusted odds ratio, 0.55; 95% confidence interval: 0.33-0.91).</p><p><strong>Conclusions: </strong>Stomach position evaluated using CT images was associated with successful initial post-pyloric EFT placement. The best cut-off value of the greater curvature of the stomach to predict the success or failure of the first attempt was spinal level L2-L3. Trial registration University Hospital Medical Information Network Clinical Trials Registry (UMIN000046986; February 28, 2022). https://center6.umin.ac.jp/cgi-open-bin/ctr/ctr_view.cgi?recptno=R000052151.</p>\",\"PeriodicalId\":16123,\"journal\":{\"name\":\"Journal of Intensive Care\",\"volume\":\"11 1\",\"pages\":\"25\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2023-05-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10228095/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Intensive Care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40560-023-00673-4\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-023-00673-4","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Stomach position evaluated using computed tomography is related to successful post-pyloric enteral feeding tube placement in critically ill patients: a retrospective observational study.
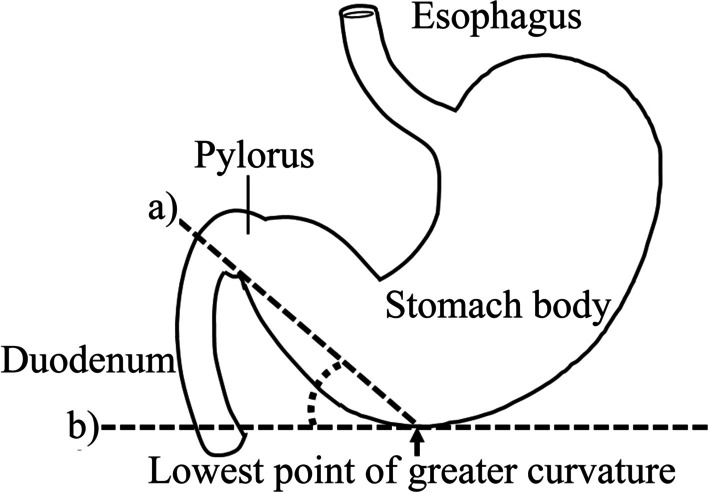
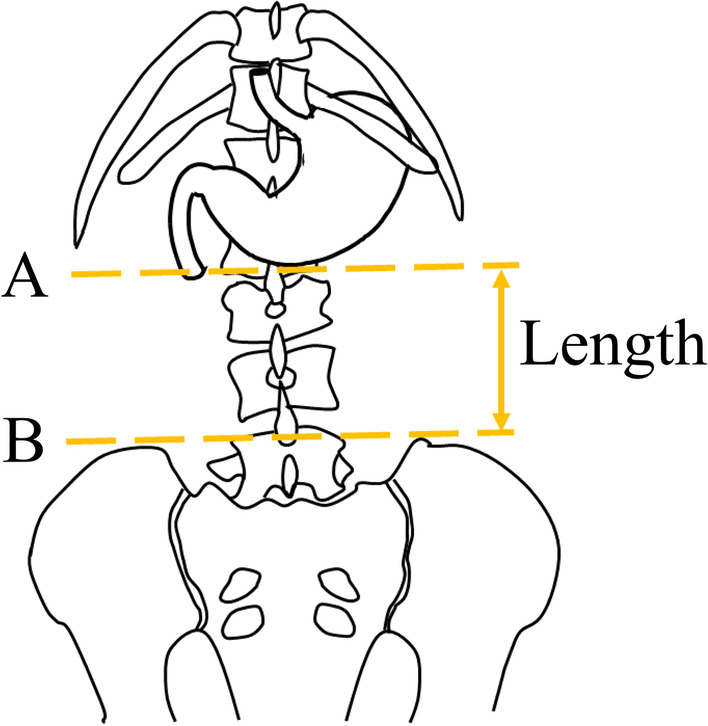
Background: Post-pyloric enteral feeding reduces respiratory complications and shortens the duration of mechanical ventilation. Blind placement of post-pyloric enteral feeding tubes (EFT) in patients with critical illnesses is often the first-line method because endoscopy or fluoroscopy cannot be easily performed at bedside; however, difficult placements regularly occur. We reported an association between the stomach position caudal to spinal level L1-L2, evaluated by abdominal radiographs after placement, and difficult placement; however, this method could not indicate difficulty before EFT placement. The aim of our study was to evaluate the association between stomach position, estimated using computed tomography (CT) images taken before the blind placement of the post-pyloric EFT, and the difficulty of EFT placement.
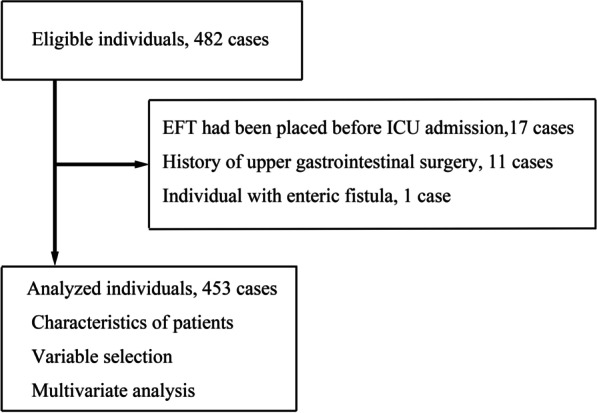
Methods: Data from patients aged ≥ 20 years who underwent post-pyloric EFT in our intensive care unit were obtained retrospectively. Logistic regression analysis was used to evaluate the association between successful initial EFT placement and explanatory variables, including stomach position estimated by CT. Two cut-off values were used: caudal to L1-L2 based on a previous study and the best cut-off value calculated by the receiver operating characteristic curve. Variable selection was performed backward stepwise using Akaike's Information Criterion.
Results: Of the total of 453 patients who were enrolled, the success rate of the initial EFT placement was 43.5%. The adjusted odds ratio for successful initial EFT placement of the stomach position caudal to L1-L2 was 0.61 (95% confidence interval: 0.41-1.07). Logistic regression analysis, including the stomach position caudal to L2-L3, calculated as the best cut-off value, indicated that stomach position was an independent factor for failure of initial EFT placement (adjusted odds ratio, 0.55; 95% confidence interval: 0.33-0.91).
Conclusions: Stomach position evaluated using CT images was associated with successful initial post-pyloric EFT placement. The best cut-off value of the greater curvature of the stomach to predict the success or failure of the first attempt was spinal level L2-L3. Trial registration University Hospital Medical Information Network Clinical Trials Registry (UMIN000046986; February 28, 2022). https://center6.umin.ac.jp/cgi-open-bin/ctr/ctr_view.cgi?recptno=R000052151.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
