{"title":"大血管闭塞患者的机械血栓切除术治疗时间超过16小时。","authors":"Takehiro Katano, Kentaro Suzuki, Ryutaro Kimura, Tomonari Saito, Yasuhiro Nishiyama, Kazumi Kimura","doi":"10.1159/000531153","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Mechanical thrombectomy (MT) has been reported to be effective within 24 h after last known well (LKW) by the DAWN (DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo) trial and within 16 h after LKW by the DEFUSE-3 (Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke 3) trial. However, there have been few reports of MT more than 16 h after LKW, and the efficacy and safety of MT more than 24 h after LKW have not yet been demonstrated. We evaluated the efficacy and safety of MT more than 16 h after LKW.</p><p><strong>Methods: </strong>Using data from the Nippon Medical School Hospital MT registry from April 2011 to August 2022, consecutive patients with anterior circulation large vessel occlusion (LVO) and prehospital modified Rankin scale (mRS) scores of 0-3 were enrolled. Patients were classified into the following three groups: early group (LKW <6 h), middle group (LKW 6-16 h), and late group (LKW >16 h). The clinical characteristics and outcomes were compared among these three groups.</p><p><strong>Results: </strong>Among 778 patients in the MT registry, 624 were enrolled. The early group included 432 patients, the middle group included 123 patients, and the late group included 69 patients. The patients had a median age of 77 years (interquartile range, 68-83), and 359 were male (57.5%). The median prehospital mRS score was 1 (interquartile range, 1-1), median National Institutes of Health Stroke Scale score on admission was 17 (interquartile range, 10-23), and median Alberta Stroke Program Early CT Score was 10 (interquartile range, 8-10). Regarding safety and efficacy, the proportions of cases with successful reperfusion (modified Thrombolysis in Cerebral Infarction score of 2b-3; 85.4% vs. 92.7% vs. 88.7%; p = 0.47), symptomatic intracranial haemorrhage (6.4% vs. 5.7% vs. 7.2%; p = 0.99), mRS score ≤3 at 90 days (52.0% vs. 60.2% vs. 44.9%; p = 0.11), and mRS score of 6 at 90 days (11.3% vs. 10.6 vs. 8.7%; p = 0.37) were not significantly different between the three groups.</p><p><strong>Conclusion: </strong>Patients who received MT more than 16 h after LKW experienced the same safety and efficacy as those who received MT at 0-16 h after LKW. MT more than 16 h after LKW may be safe and effective for stroke patients with LVO.</p>","PeriodicalId":45709,"journal":{"name":"Cerebrovascular Diseases Extra","volume":" ","pages":"69-74"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9f/9a/cee-2023-0013-0001-531153.PMC10601849.pdf","citationCount":"0","resultStr":"{\"title\":\"Mechanical Thrombectomy Treatment More than 16 h after Last Known Well for Patients with Large Vessel Occlusion.\",\"authors\":\"Takehiro Katano, Kentaro Suzuki, Ryutaro Kimura, Tomonari Saito, Yasuhiro Nishiyama, Kazumi Kimura\",\"doi\":\"10.1159/000531153\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Mechanical thrombectomy (MT) has been reported to be effective within 24 h after last known well (LKW) by the DAWN (DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo) trial and within 16 h after LKW by the DEFUSE-3 (Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke 3) trial. However, there have been few reports of MT more than 16 h after LKW, and the efficacy and safety of MT more than 24 h after LKW have not yet been demonstrated. We evaluated the efficacy and safety of MT more than 16 h after LKW.</p><p><strong>Methods: </strong>Using data from the Nippon Medical School Hospital MT registry from April 2011 to August 2022, consecutive patients with anterior circulation large vessel occlusion (LVO) and prehospital modified Rankin scale (mRS) scores of 0-3 were enrolled. Patients were classified into the following three groups: early group (LKW <6 h), middle group (LKW 6-16 h), and late group (LKW >16 h). The clinical characteristics and outcomes were compared among these three groups.</p><p><strong>Results: </strong>Among 778 patients in the MT registry, 624 were enrolled. The early group included 432 patients, the middle group included 123 patients, and the late group included 69 patients. The patients had a median age of 77 years (interquartile range, 68-83), and 359 were male (57.5%). The median prehospital mRS score was 1 (interquartile range, 1-1), median National Institutes of Health Stroke Scale score on admission was 17 (interquartile range, 10-23), and median Alberta Stroke Program Early CT Score was 10 (interquartile range, 8-10). Regarding safety and efficacy, the proportions of cases with successful reperfusion (modified Thrombolysis in Cerebral Infarction score of 2b-3; 85.4% vs. 92.7% vs. 88.7%; p = 0.47), symptomatic intracranial haemorrhage (6.4% vs. 5.7% vs. 7.2%; p = 0.99), mRS score ≤3 at 90 days (52.0% vs. 60.2% vs. 44.9%; p = 0.11), and mRS score of 6 at 90 days (11.3% vs. 10.6 vs. 8.7%; p = 0.37) were not significantly different between the three groups.</p><p><strong>Conclusion: </strong>Patients who received MT more than 16 h after LKW experienced the same safety and efficacy as those who received MT at 0-16 h after LKW. MT more than 16 h after LKW may be safe and effective for stroke patients with LVO.</p>\",\"PeriodicalId\":45709,\"journal\":{\"name\":\"Cerebrovascular Diseases Extra\",\"volume\":\" \",\"pages\":\"69-74\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9f/9a/cee-2023-0013-0001-531153.PMC10601849.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cerebrovascular Diseases Extra\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000531153\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/6/1 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebrovascular Diseases Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000531153","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/1 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Mechanical Thrombectomy Treatment More than 16 h after Last Known Well for Patients with Large Vessel Occlusion.
Introduction: Mechanical thrombectomy (MT) has been reported to be effective within 24 h after last known well (LKW) by the DAWN (DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo) trial and within 16 h after LKW by the DEFUSE-3 (Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke 3) trial. However, there have been few reports of MT more than 16 h after LKW, and the efficacy and safety of MT more than 24 h after LKW have not yet been demonstrated. We evaluated the efficacy and safety of MT more than 16 h after LKW.
Methods: Using data from the Nippon Medical School Hospital MT registry from April 2011 to August 2022, consecutive patients with anterior circulation large vessel occlusion (LVO) and prehospital modified Rankin scale (mRS) scores of 0-3 were enrolled. Patients were classified into the following three groups: early group (LKW <6 h), middle group (LKW 6-16 h), and late group (LKW >16 h). The clinical characteristics and outcomes were compared among these three groups.
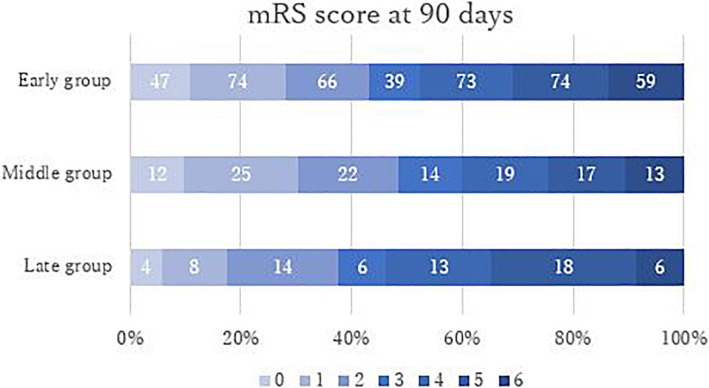
Results: Among 778 patients in the MT registry, 624 were enrolled. The early group included 432 patients, the middle group included 123 patients, and the late group included 69 patients. The patients had a median age of 77 years (interquartile range, 68-83), and 359 were male (57.5%). The median prehospital mRS score was 1 (interquartile range, 1-1), median National Institutes of Health Stroke Scale score on admission was 17 (interquartile range, 10-23), and median Alberta Stroke Program Early CT Score was 10 (interquartile range, 8-10). Regarding safety and efficacy, the proportions of cases with successful reperfusion (modified Thrombolysis in Cerebral Infarction score of 2b-3; 85.4% vs. 92.7% vs. 88.7%; p = 0.47), symptomatic intracranial haemorrhage (6.4% vs. 5.7% vs. 7.2%; p = 0.99), mRS score ≤3 at 90 days (52.0% vs. 60.2% vs. 44.9%; p = 0.11), and mRS score of 6 at 90 days (11.3% vs. 10.6 vs. 8.7%; p = 0.37) were not significantly different between the three groups.
Conclusion: Patients who received MT more than 16 h after LKW experienced the same safety and efficacy as those who received MT at 0-16 h after LKW. MT more than 16 h after LKW may be safe and effective for stroke patients with LVO.
期刊介绍:
This open access and online-only journal publishes original articles covering the entire spectrum of stroke and cerebrovascular research, drawing from a variety of specialties such as neurology, internal medicine, surgery, radiology, epidemiology, cardiology, hematology, psychology and rehabilitation. Offering an international forum, it meets the growing need for sophisticated, up-to-date scientific information on clinical data, diagnostic testing, and therapeutic issues. The journal publishes original contributions, reviews of selected topics as well as clinical investigative studies. All aspects related to clinical advances are considered, while purely experimental work appears only if directly relevant to clinical issues. Cerebrovascular Diseases Extra provides additional contents based on reviewed and accepted submissions to the main journal Cerebrovascular Diseases.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
