{"title":"吉马医疗中心治疗儿童癌症的成本和成本效益。","authors":"Idiris Genemo, Temesgen Kabeta Chala, Diriba Fufa Hordofa, Shimeles Ololo Sinkie","doi":"10.2147/CEOR.S395170","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>More than 70% of childhood cancer patients die in Sub-Saharan African countries due to a lack of access. Additionally establishing a childhood cancer treatment service is perceived as expensive by the decision-makers of LMICs. However, there is a paucity of evidence on the actual cost and cost-effectiveness of this service in LMICs including Ethiopia. This study provides context-relevant evidence to consider childhood cancer treatment in the healthcare priority settings in Ethiopia and other LMICs.</p><p><strong>Methods: </strong>Newly admitted case files of children for the year 2020/21 were reviewed. The cost was analyzed from the provider's perspective. The effectiveness was calculated using DALY averted based on the 5 years of survival rates, which is estimated from the 1-year survival rate of Kaplan-Meier output. The do-nothing was our comparator, and we assumed no cost (zero cost) will be incurred for the comparator. To account for sensitivity analyses, we varied the discount rate, 5-year survival rate, and life expectancy.</p><p><strong>Results: </strong>During the study period, 101 children were treated in the unit. The total annual and unit cost to give treatment to childhood cancer patients was estimated at $279,648 and $2769, respectively. The highest per-patient annual unit cost of treatment was Hodgkin's lymphoma ($6252), while Retinoblastoma ($1520) was the least. The cost per DALY averted was $193, which is significantly less than Ethiopia's GDP per capita ($936.3). The results remained very cost-effective in sensitivity analyses.</p><p><strong>Conclusion: </strong>Childhood cancer treatment is very cost-effective in Ethiopia as per WHO-CHOICE thresholds even in a conservative adjustment of assumptions. Therefore, to enhance and improve children's health, childhood cancer should get a better concern in health priority.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"15 ","pages":"433-442"},"PeriodicalIF":2.2000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f0/9a/ceor-15-433.PMC10257924.pdf","citationCount":"0","resultStr":"{\"title\":\"Cost and Cost-Effectiveness of Treating Childhood Cancer at Jimma Medical Center.\",\"authors\":\"Idiris Genemo, Temesgen Kabeta Chala, Diriba Fufa Hordofa, Shimeles Ololo Sinkie\",\"doi\":\"10.2147/CEOR.S395170\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>More than 70% of childhood cancer patients die in Sub-Saharan African countries due to a lack of access. Additionally establishing a childhood cancer treatment service is perceived as expensive by the decision-makers of LMICs. However, there is a paucity of evidence on the actual cost and cost-effectiveness of this service in LMICs including Ethiopia. This study provides context-relevant evidence to consider childhood cancer treatment in the healthcare priority settings in Ethiopia and other LMICs.</p><p><strong>Methods: </strong>Newly admitted case files of children for the year 2020/21 were reviewed. The cost was analyzed from the provider's perspective. The effectiveness was calculated using DALY averted based on the 5 years of survival rates, which is estimated from the 1-year survival rate of Kaplan-Meier output. The do-nothing was our comparator, and we assumed no cost (zero cost) will be incurred for the comparator. To account for sensitivity analyses, we varied the discount rate, 5-year survival rate, and life expectancy.</p><p><strong>Results: </strong>During the study period, 101 children were treated in the unit. The total annual and unit cost to give treatment to childhood cancer patients was estimated at $279,648 and $2769, respectively. The highest per-patient annual unit cost of treatment was Hodgkin's lymphoma ($6252), while Retinoblastoma ($1520) was the least. The cost per DALY averted was $193, which is significantly less than Ethiopia's GDP per capita ($936.3). The results remained very cost-effective in sensitivity analyses.</p><p><strong>Conclusion: </strong>Childhood cancer treatment is very cost-effective in Ethiopia as per WHO-CHOICE thresholds even in a conservative adjustment of assumptions. Therefore, to enhance and improve children's health, childhood cancer should get a better concern in health priority.</p>\",\"PeriodicalId\":47313,\"journal\":{\"name\":\"ClinicoEconomics and Outcomes Research\",\"volume\":\"15 \",\"pages\":\"433-442\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f0/9a/ceor-15-433.PMC10257924.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ClinicoEconomics and Outcomes Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/CEOR.S395170\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S395170","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Cost and Cost-Effectiveness of Treating Childhood Cancer at Jimma Medical Center.
Background: More than 70% of childhood cancer patients die in Sub-Saharan African countries due to a lack of access. Additionally establishing a childhood cancer treatment service is perceived as expensive by the decision-makers of LMICs. However, there is a paucity of evidence on the actual cost and cost-effectiveness of this service in LMICs including Ethiopia. This study provides context-relevant evidence to consider childhood cancer treatment in the healthcare priority settings in Ethiopia and other LMICs.
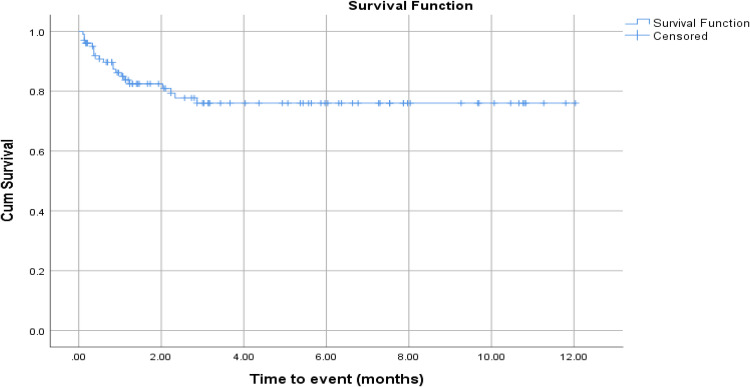
Methods: Newly admitted case files of children for the year 2020/21 were reviewed. The cost was analyzed from the provider's perspective. The effectiveness was calculated using DALY averted based on the 5 years of survival rates, which is estimated from the 1-year survival rate of Kaplan-Meier output. The do-nothing was our comparator, and we assumed no cost (zero cost) will be incurred for the comparator. To account for sensitivity analyses, we varied the discount rate, 5-year survival rate, and life expectancy.
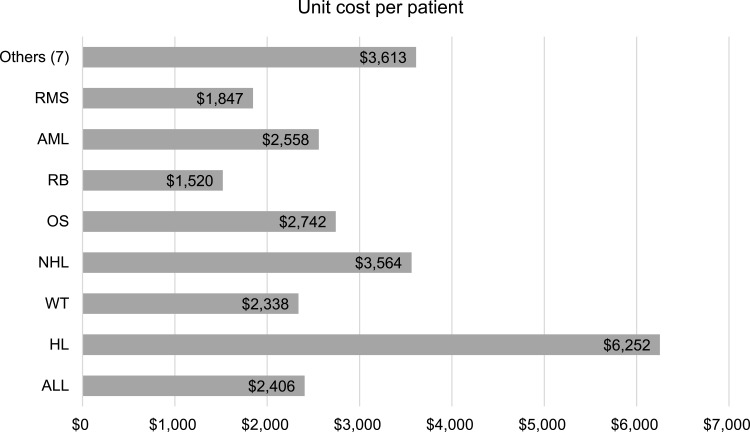
Results: During the study period, 101 children were treated in the unit. The total annual and unit cost to give treatment to childhood cancer patients was estimated at $279,648 and $2769, respectively. The highest per-patient annual unit cost of treatment was Hodgkin's lymphoma ($6252), while Retinoblastoma ($1520) was the least. The cost per DALY averted was $193, which is significantly less than Ethiopia's GDP per capita ($936.3). The results remained very cost-effective in sensitivity analyses.
Conclusion: Childhood cancer treatment is very cost-effective in Ethiopia as per WHO-CHOICE thresholds even in a conservative adjustment of assumptions. Therefore, to enhance and improve children's health, childhood cancer should get a better concern in health priority.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
