John Taylor, Sohiub N Assaf, Abdallah N Assaf, Eric Heidel, William Mahlow, Raj Baljepally
{"title":"阻塞性睡眠呼吸暂停作为心房颤动患者肺静脉隔离期间诱发心房颤动的预测因素:临床意义和随访结果。","authors":"John Taylor, Sohiub N Assaf, Abdallah N Assaf, Eric Heidel, William Mahlow, Raj Baljepally","doi":"10.14740/cr1491","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Atrial fibrillation (AF) and atrial flutter (AFL) often coexist in patients and may lead to severe symptoms and complications. Despite their coexistence, prophylactic cavotricuspid isthmus (CTI) ablation has failed to reduce the incidence of recurrent AF or new onset AFL. In contrast, the presence of inducible AFL during pulmonary vein isolation (PVI) has been shown to be predictive of symptomatic AFL during follow-up. However, the potential role of obstructive sleep apnea (OSA) as a predictor of inducible AFL during PVI in patients with AF remains unclear. Therefore, this study aimed to examine the potential role of OSA as a predictor of inducible AFL during PVI in patients with AF and reexamine the clinical significance of inducible AFL during PVI in terms of recurrent AFL or AF during follow-up.</p><p><strong>Methods: </strong>We conducted a single-center, non-randomized retrospective study on patients who underwent PVI between October 2013 and December 2020. A total of 192 patients were included in the study after screening 257 patients for exclusion criteria, which included a previous history of AFL or previous PVI or Maze procedure. All patients underwent a transesophageal echocardiogram (TEE) prior to their ablation to rule out a left atrial appendage thrombus. The PVI was performed using both fluoroscopic and electroanatomic mapping derived from intracardiac echocardiography. After the confirmation of PVI, additional electrophysiology (EP) testing was performed. AFL was classified as typical or atypical based on the origin and activation pattern. Descriptive and frequency statistics were performed to describe the demographic and clinical characteristics of the sample, and Chi-square and Fisher's exact tests were used to compare independent groups on categorical outcomes. Logistic regression analysis was performed to adjust for confounding variables. The study was approved by the Institutional Review Board, and informed consent was waived given the retrospective nature of the study.</p><p><strong>Results: </strong>Of the 192 patients included in the study, 52% (n = 100) had inducible AFL after PVI, with 43% (n = 82) having typical right AFL. Bivariate analysis showed statistically significant differences between the groups for OSA (P = 0.04) and persistent AF (P = 0.047) when examining the outcome of any inducible AFL. Similarly, only OSA (P = 0.04) and persistent AF (P = 0.043) were significant when examining the outcome of typical right AFL. Multivariate analysis showed that only OSA was significantly associated with any inducible AFL after controlling for other variables (adjusted odds ratio (AOR) = 1.92, 95% confidence interval (CI): 1.003 - 3.69, P = 0.049). Of the 100 patients with inducible AFL, 89 underwent additional ablation for AFL prior to completion of their procedure. At 1 year, the rates of recurrence for AF, AFL, and either AF or AFL were 31%, 10%, and 38%, respectively. There was no significant difference in the rates of recurrence of AF, AFL, or either AF/AFL at 1 year when accounting for the presence of inducible AFL or the efficacy of additional AFL ablation.</p><p><strong>Conclusions: </strong>In conclusion, our study found a high incidence of inducible AFL during PVI, particularly among patients with OSA. However, the clinical significance of inducible AFL in relation to the recurrence rates of AF or AFL at 1-year post-PVI remains unclear. Our findings suggest that successful ablation of inducible AFL during PVI may not provide clinical benefit in reducing AF or AFL recurrence. To establish the clinical significance of inducible AFL during PVI in various patient populations, further prospective studies with larger sample sizes and longer follow-up periods are necessary.</p>","PeriodicalId":9424,"journal":{"name":"Cardiology Research","volume":"14 3","pages":"183-191"},"PeriodicalIF":1.4000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/97/76/cr-14-183.PMC10257505.pdf","citationCount":"0","resultStr":"{\"title\":\"Obstructive Sleep Apnea as a Predictor of Inducible Atrial Flutter During Pulmonary Vein Isolation in Patients With Atrial Fibrillation: Clinical Significance and Follow-Up Outcomes.\",\"authors\":\"John Taylor, Sohiub N Assaf, Abdallah N Assaf, Eric Heidel, William Mahlow, Raj Baljepally\",\"doi\":\"10.14740/cr1491\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Atrial fibrillation (AF) and atrial flutter (AFL) often coexist in patients and may lead to severe symptoms and complications. Despite their coexistence, prophylactic cavotricuspid isthmus (CTI) ablation has failed to reduce the incidence of recurrent AF or new onset AFL. In contrast, the presence of inducible AFL during pulmonary vein isolation (PVI) has been shown to be predictive of symptomatic AFL during follow-up. However, the potential role of obstructive sleep apnea (OSA) as a predictor of inducible AFL during PVI in patients with AF remains unclear. Therefore, this study aimed to examine the potential role of OSA as a predictor of inducible AFL during PVI in patients with AF and reexamine the clinical significance of inducible AFL during PVI in terms of recurrent AFL or AF during follow-up.</p><p><strong>Methods: </strong>We conducted a single-center, non-randomized retrospective study on patients who underwent PVI between October 2013 and December 2020. A total of 192 patients were included in the study after screening 257 patients for exclusion criteria, which included a previous history of AFL or previous PVI or Maze procedure. All patients underwent a transesophageal echocardiogram (TEE) prior to their ablation to rule out a left atrial appendage thrombus. The PVI was performed using both fluoroscopic and electroanatomic mapping derived from intracardiac echocardiography. After the confirmation of PVI, additional electrophysiology (EP) testing was performed. AFL was classified as typical or atypical based on the origin and activation pattern. Descriptive and frequency statistics were performed to describe the demographic and clinical characteristics of the sample, and Chi-square and Fisher's exact tests were used to compare independent groups on categorical outcomes. Logistic regression analysis was performed to adjust for confounding variables. The study was approved by the Institutional Review Board, and informed consent was waived given the retrospective nature of the study.</p><p><strong>Results: </strong>Of the 192 patients included in the study, 52% (n = 100) had inducible AFL after PVI, with 43% (n = 82) having typical right AFL. Bivariate analysis showed statistically significant differences between the groups for OSA (P = 0.04) and persistent AF (P = 0.047) when examining the outcome of any inducible AFL. Similarly, only OSA (P = 0.04) and persistent AF (P = 0.043) were significant when examining the outcome of typical right AFL. Multivariate analysis showed that only OSA was significantly associated with any inducible AFL after controlling for other variables (adjusted odds ratio (AOR) = 1.92, 95% confidence interval (CI): 1.003 - 3.69, P = 0.049). Of the 100 patients with inducible AFL, 89 underwent additional ablation for AFL prior to completion of their procedure. At 1 year, the rates of recurrence for AF, AFL, and either AF or AFL were 31%, 10%, and 38%, respectively. There was no significant difference in the rates of recurrence of AF, AFL, or either AF/AFL at 1 year when accounting for the presence of inducible AFL or the efficacy of additional AFL ablation.</p><p><strong>Conclusions: </strong>In conclusion, our study found a high incidence of inducible AFL during PVI, particularly among patients with OSA. However, the clinical significance of inducible AFL in relation to the recurrence rates of AF or AFL at 1-year post-PVI remains unclear. Our findings suggest that successful ablation of inducible AFL during PVI may not provide clinical benefit in reducing AF or AFL recurrence. To establish the clinical significance of inducible AFL during PVI in various patient populations, further prospective studies with larger sample sizes and longer follow-up periods are necessary.</p>\",\"PeriodicalId\":9424,\"journal\":{\"name\":\"Cardiology Research\",\"volume\":\"14 3\",\"pages\":\"183-191\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/97/76/cr-14-183.PMC10257505.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/cr1491\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/5/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/cr1491","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/5/26 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Obstructive Sleep Apnea as a Predictor of Inducible Atrial Flutter During Pulmonary Vein Isolation in Patients With Atrial Fibrillation: Clinical Significance and Follow-Up Outcomes.
Background: Atrial fibrillation (AF) and atrial flutter (AFL) often coexist in patients and may lead to severe symptoms and complications. Despite their coexistence, prophylactic cavotricuspid isthmus (CTI) ablation has failed to reduce the incidence of recurrent AF or new onset AFL. In contrast, the presence of inducible AFL during pulmonary vein isolation (PVI) has been shown to be predictive of symptomatic AFL during follow-up. However, the potential role of obstructive sleep apnea (OSA) as a predictor of inducible AFL during PVI in patients with AF remains unclear. Therefore, this study aimed to examine the potential role of OSA as a predictor of inducible AFL during PVI in patients with AF and reexamine the clinical significance of inducible AFL during PVI in terms of recurrent AFL or AF during follow-up.
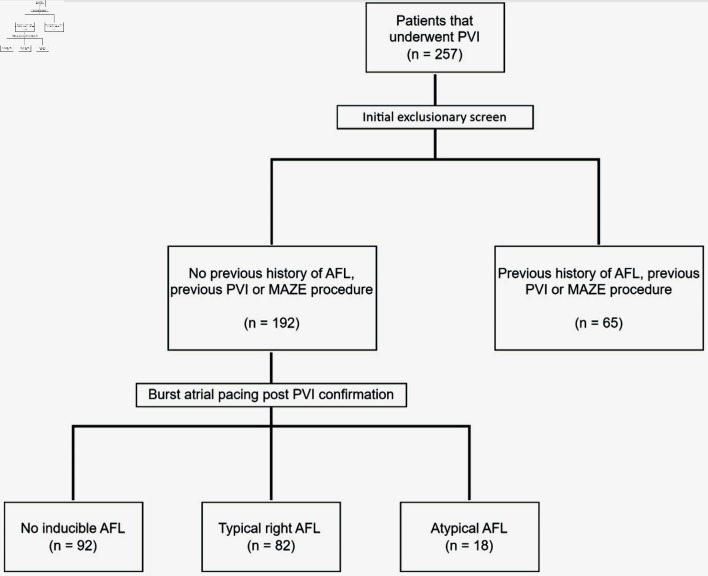
Methods: We conducted a single-center, non-randomized retrospective study on patients who underwent PVI between October 2013 and December 2020. A total of 192 patients were included in the study after screening 257 patients for exclusion criteria, which included a previous history of AFL or previous PVI or Maze procedure. All patients underwent a transesophageal echocardiogram (TEE) prior to their ablation to rule out a left atrial appendage thrombus. The PVI was performed using both fluoroscopic and electroanatomic mapping derived from intracardiac echocardiography. After the confirmation of PVI, additional electrophysiology (EP) testing was performed. AFL was classified as typical or atypical based on the origin and activation pattern. Descriptive and frequency statistics were performed to describe the demographic and clinical characteristics of the sample, and Chi-square and Fisher's exact tests were used to compare independent groups on categorical outcomes. Logistic regression analysis was performed to adjust for confounding variables. The study was approved by the Institutional Review Board, and informed consent was waived given the retrospective nature of the study.
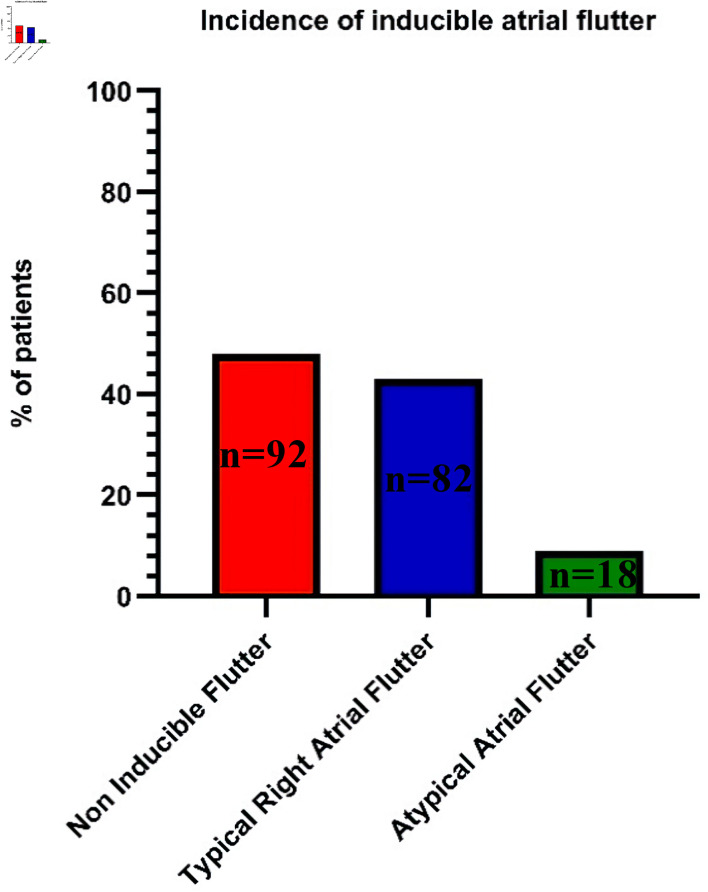
Results: Of the 192 patients included in the study, 52% (n = 100) had inducible AFL after PVI, with 43% (n = 82) having typical right AFL. Bivariate analysis showed statistically significant differences between the groups for OSA (P = 0.04) and persistent AF (P = 0.047) when examining the outcome of any inducible AFL. Similarly, only OSA (P = 0.04) and persistent AF (P = 0.043) were significant when examining the outcome of typical right AFL. Multivariate analysis showed that only OSA was significantly associated with any inducible AFL after controlling for other variables (adjusted odds ratio (AOR) = 1.92, 95% confidence interval (CI): 1.003 - 3.69, P = 0.049). Of the 100 patients with inducible AFL, 89 underwent additional ablation for AFL prior to completion of their procedure. At 1 year, the rates of recurrence for AF, AFL, and either AF or AFL were 31%, 10%, and 38%, respectively. There was no significant difference in the rates of recurrence of AF, AFL, or either AF/AFL at 1 year when accounting for the presence of inducible AFL or the efficacy of additional AFL ablation.
Conclusions: In conclusion, our study found a high incidence of inducible AFL during PVI, particularly among patients with OSA. However, the clinical significance of inducible AFL in relation to the recurrence rates of AF or AFL at 1-year post-PVI remains unclear. Our findings suggest that successful ablation of inducible AFL during PVI may not provide clinical benefit in reducing AF or AFL recurrence. To establish the clinical significance of inducible AFL during PVI in various patient populations, further prospective studies with larger sample sizes and longer follow-up periods are necessary.
期刊介绍:
Cardiology Research is an open access, peer-reviewed, international journal. All submissions relating to basic research and clinical practice of cardiology and cardiovascular medicine are in this journal''s scope. This journal focuses on publishing original research and observations in all cardiovascular medicine aspects. Manuscript types include original article, review, case report, short communication, book review, letter to the editor.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
