{"title":"腰椎骨内侵袭性神经鞘瘤1例报告。","authors":"Takashi Hirai, Toshitaka Yoshii, Hiroyuki Inose, Yu Matsukura, Yuki Funauchi, Satoru Egawa, Kurando Utagawa, Jun Hashimoto, Mariko Nishizawa, Kohei Yamamoto, Atsushi Okawa","doi":"10.22603/ssrr.2022-0168","DOIUrl":null,"url":null,"abstract":"A 66-year-old man was presented at another hospital with increased urinary frequency and lower limb numbness and was diagnosed with lumbar spinal canal stenosis (LSCS). Although he received prostaglandin as treatment for cauda equine caused by LSCS, the symptoms did not resolve. Results of the subsequent magnetic resonance imaging (MRI) revealed a solid tumor in the fifth lumbar vertebra (L5) and spinal canal (Fig. 1A-E). Interestingly, the tumor did not extend to the intervertebral foramen and did not form a dumbbell shape. He was referred to our hospital for surgical treatment. A computed tomography scan after myelogram was performed to investigate the dural sac in the spinal canal. The tumor was observed to completely fill the canal such that the dural sac was not detectable (Fig. 1F and G). There was no other tumor in the canal. Transpedicular biopsy revealed a cluster of spindle cells and the partial presence of a necrotic lesion, which was suspected to be intraosseous schwannoma. Because the facet joint at L5/S1 was disrupted due to scalloping caused by the tumor, L4-S1 posterior lateral fusion (PLF) with instrumentation as well as L5 and S1 laminectomy were performed to remove the giant tumor. After fenestration, remarkable compression of the dural sac caused by the giant tumor was confirmed (Fig. 2A). The tumor contents were completely removed using an ultrasonic aspirator (CUSA Clarity, Integra LifeSciences, Tokyo, Japan). Although foraminotomy was performed after a sufficient mass reduction in order to identify the inlet nerve root, we could not locate the nerve tissue that resembled a spinal nerve root. Finally, a capsule of the tumor and an adhesive band linked to the right L5 nerve root were isolated (Fig. 2B). Histological examination revealed schwannoma with 2.1% Ki-67-positive cells (Fig. 2C). Artificial bone cement containing polymethyl methacrylate (SpinePlex; Stryker Corporation, Kalamazoo, MI) was placed into the defect, and PLF was performed (Fig. 3A-D). Postoperative MRI showed that the tumor was completely removed, while scar tissue remained in front of the dural sac (Fig. 3E). His lower limb numbness gradually improved, and there was no tumor recurrence during the 2-year follow-up period; however, the urinary disorder persisted. Clinically, although schwannoma is a benign neural tumor and can occur anywhere in the body, intraosseous presentation is extremely rare, accounting for 0.2% of primary tumors. Notably, only 10 cases with aggressive intraosseous schwannoma in the lumbar spine have been reported to date (Table 1). Although spinal nerve sheath schwannoma often grows into the spinal canal and intervertebral foramen, thereby forming a dumbbell tumor usually with sclerotic and clear margins, aggressive intraosseous schwannoma can lead to invasive and osteolytic bone destruction in the vertebrae. Therefore, it is important in terms of radiological evaluation to understand the difficulty in differentiating between malignant tumors and osteolytic lesions caused by aggressive intraosseous schwannoma. Fortunately, in most cases, total resection is performed with posterior instrumentation, and there is no recurrence during the approximately","PeriodicalId":22253,"journal":{"name":"Spine Surgery and Related Research","volume":null,"pages":null},"PeriodicalIF":1.2000,"publicationDate":"2023-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b7/dd/2432-261X-7-0288.PMC10257963.pdf","citationCount":"0","resultStr":"{\"title\":\"Intraosseous Aggressive Schwannoma in the Lumbar Spine: A Case Report.\",\"authors\":\"Takashi Hirai, Toshitaka Yoshii, Hiroyuki Inose, Yu Matsukura, Yuki Funauchi, Satoru Egawa, Kurando Utagawa, Jun Hashimoto, Mariko Nishizawa, Kohei Yamamoto, Atsushi Okawa\",\"doi\":\"10.22603/ssrr.2022-0168\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"A 66-year-old man was presented at another hospital with increased urinary frequency and lower limb numbness and was diagnosed with lumbar spinal canal stenosis (LSCS). Although he received prostaglandin as treatment for cauda equine caused by LSCS, the symptoms did not resolve. Results of the subsequent magnetic resonance imaging (MRI) revealed a solid tumor in the fifth lumbar vertebra (L5) and spinal canal (Fig. 1A-E). Interestingly, the tumor did not extend to the intervertebral foramen and did not form a dumbbell shape. He was referred to our hospital for surgical treatment. A computed tomography scan after myelogram was performed to investigate the dural sac in the spinal canal. The tumor was observed to completely fill the canal such that the dural sac was not detectable (Fig. 1F and G). There was no other tumor in the canal. Transpedicular biopsy revealed a cluster of spindle cells and the partial presence of a necrotic lesion, which was suspected to be intraosseous schwannoma. Because the facet joint at L5/S1 was disrupted due to scalloping caused by the tumor, L4-S1 posterior lateral fusion (PLF) with instrumentation as well as L5 and S1 laminectomy were performed to remove the giant tumor. After fenestration, remarkable compression of the dural sac caused by the giant tumor was confirmed (Fig. 2A). The tumor contents were completely removed using an ultrasonic aspirator (CUSA Clarity, Integra LifeSciences, Tokyo, Japan). Although foraminotomy was performed after a sufficient mass reduction in order to identify the inlet nerve root, we could not locate the nerve tissue that resembled a spinal nerve root. Finally, a capsule of the tumor and an adhesive band linked to the right L5 nerve root were isolated (Fig. 2B). Histological examination revealed schwannoma with 2.1% Ki-67-positive cells (Fig. 2C). Artificial bone cement containing polymethyl methacrylate (SpinePlex; Stryker Corporation, Kalamazoo, MI) was placed into the defect, and PLF was performed (Fig. 3A-D). Postoperative MRI showed that the tumor was completely removed, while scar tissue remained in front of the dural sac (Fig. 3E). His lower limb numbness gradually improved, and there was no tumor recurrence during the 2-year follow-up period; however, the urinary disorder persisted. Clinically, although schwannoma is a benign neural tumor and can occur anywhere in the body, intraosseous presentation is extremely rare, accounting for 0.2% of primary tumors. Notably, only 10 cases with aggressive intraosseous schwannoma in the lumbar spine have been reported to date (Table 1). Although spinal nerve sheath schwannoma often grows into the spinal canal and intervertebral foramen, thereby forming a dumbbell tumor usually with sclerotic and clear margins, aggressive intraosseous schwannoma can lead to invasive and osteolytic bone destruction in the vertebrae. Therefore, it is important in terms of radiological evaluation to understand the difficulty in differentiating between malignant tumors and osteolytic lesions caused by aggressive intraosseous schwannoma. Fortunately, in most cases, total resection is performed with posterior instrumentation, and there is no recurrence during the approximately\",\"PeriodicalId\":22253,\"journal\":{\"name\":\"Spine Surgery and Related Research\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-05-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b7/dd/2432-261X-7-0288.PMC10257963.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spine Surgery and Related Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22603/ssrr.2022-0168\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine Surgery and Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22603/ssrr.2022-0168","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Intraosseous Aggressive Schwannoma in the Lumbar Spine: A Case Report.
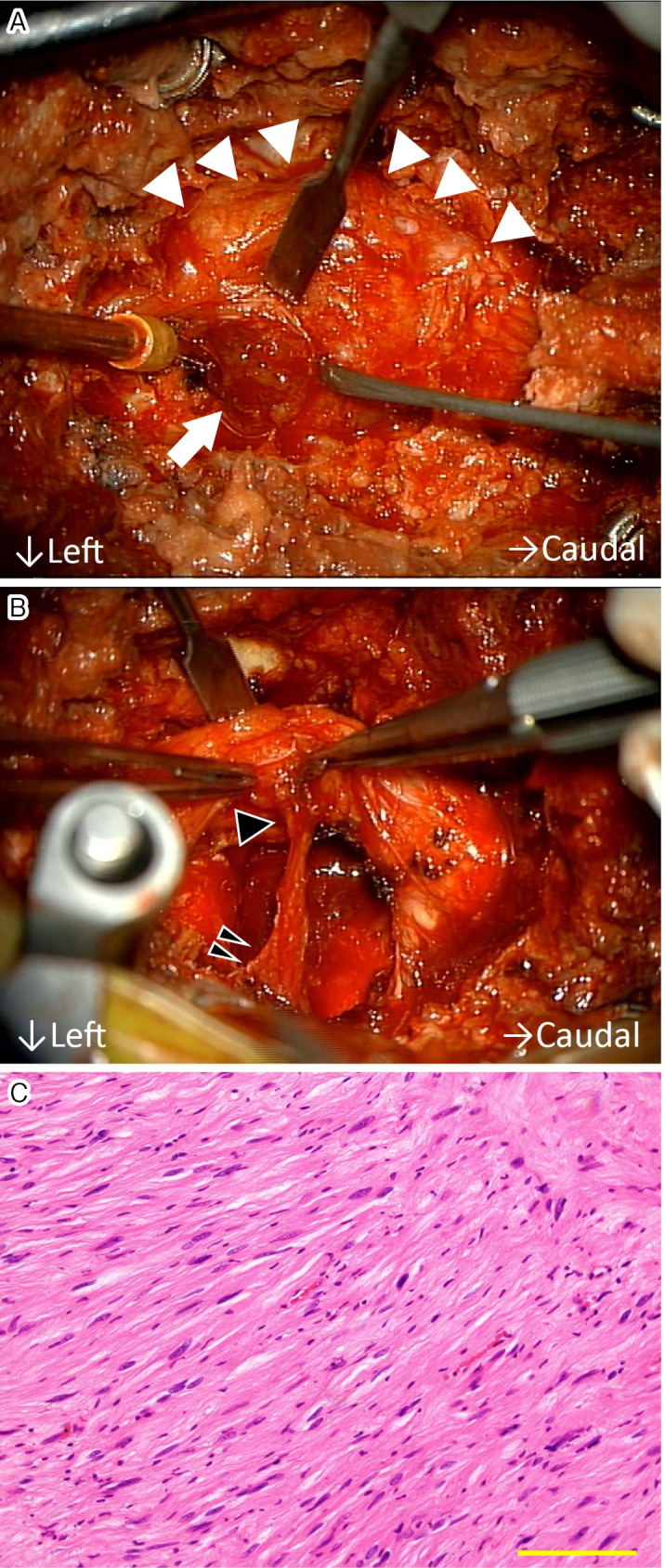
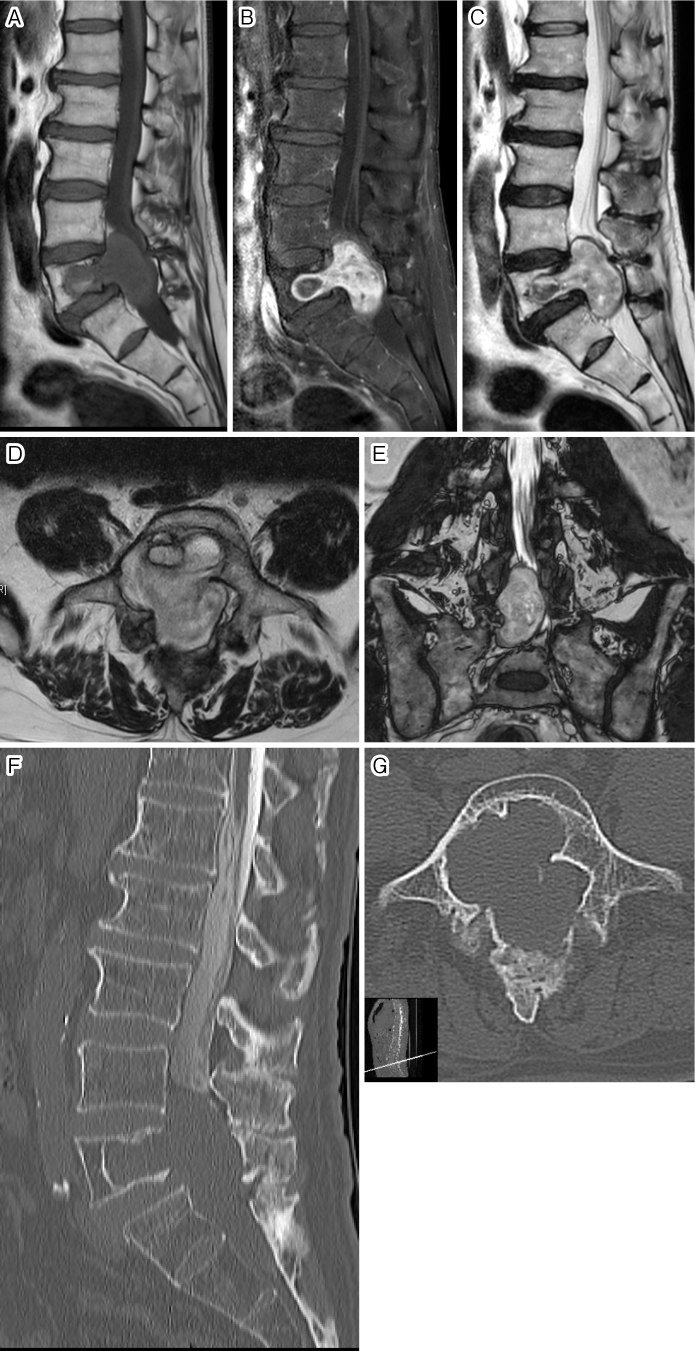
A 66-year-old man was presented at another hospital with increased urinary frequency and lower limb numbness and was diagnosed with lumbar spinal canal stenosis (LSCS). Although he received prostaglandin as treatment for cauda equine caused by LSCS, the symptoms did not resolve. Results of the subsequent magnetic resonance imaging (MRI) revealed a solid tumor in the fifth lumbar vertebra (L5) and spinal canal (Fig. 1A-E). Interestingly, the tumor did not extend to the intervertebral foramen and did not form a dumbbell shape. He was referred to our hospital for surgical treatment. A computed tomography scan after myelogram was performed to investigate the dural sac in the spinal canal. The tumor was observed to completely fill the canal such that the dural sac was not detectable (Fig. 1F and G). There was no other tumor in the canal. Transpedicular biopsy revealed a cluster of spindle cells and the partial presence of a necrotic lesion, which was suspected to be intraosseous schwannoma. Because the facet joint at L5/S1 was disrupted due to scalloping caused by the tumor, L4-S1 posterior lateral fusion (PLF) with instrumentation as well as L5 and S1 laminectomy were performed to remove the giant tumor. After fenestration, remarkable compression of the dural sac caused by the giant tumor was confirmed (Fig. 2A). The tumor contents were completely removed using an ultrasonic aspirator (CUSA Clarity, Integra LifeSciences, Tokyo, Japan). Although foraminotomy was performed after a sufficient mass reduction in order to identify the inlet nerve root, we could not locate the nerve tissue that resembled a spinal nerve root. Finally, a capsule of the tumor and an adhesive band linked to the right L5 nerve root were isolated (Fig. 2B). Histological examination revealed schwannoma with 2.1% Ki-67-positive cells (Fig. 2C). Artificial bone cement containing polymethyl methacrylate (SpinePlex; Stryker Corporation, Kalamazoo, MI) was placed into the defect, and PLF was performed (Fig. 3A-D). Postoperative MRI showed that the tumor was completely removed, while scar tissue remained in front of the dural sac (Fig. 3E). His lower limb numbness gradually improved, and there was no tumor recurrence during the 2-year follow-up period; however, the urinary disorder persisted. Clinically, although schwannoma is a benign neural tumor and can occur anywhere in the body, intraosseous presentation is extremely rare, accounting for 0.2% of primary tumors. Notably, only 10 cases with aggressive intraosseous schwannoma in the lumbar spine have been reported to date (Table 1). Although spinal nerve sheath schwannoma often grows into the spinal canal and intervertebral foramen, thereby forming a dumbbell tumor usually with sclerotic and clear margins, aggressive intraosseous schwannoma can lead to invasive and osteolytic bone destruction in the vertebrae. Therefore, it is important in terms of radiological evaluation to understand the difficulty in differentiating between malignant tumors and osteolytic lesions caused by aggressive intraosseous schwannoma. Fortunately, in most cases, total resection is performed with posterior instrumentation, and there is no recurrence during the approximately




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
