Delphine Szecel, Marie Lamberigts, Filip Rega, Peter Verbrugghe, Christophe Dubois, Bart Meuris
{"title":"避免无缝线瓣膜过大,可降低经瓣梯度,减少术后永久性起搏器植入。","authors":"Delphine Szecel, Marie Lamberigts, Filip Rega, Peter Verbrugghe, Christophe Dubois, Bart Meuris","doi":"10.1093/icvts/ivac157","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The aim of this study was to evaluate the impact of changing the sizing strategy in aortic valve replacement using the Perceval sutureless prosthesis on haemodynamic outcomes and postoperative pacemaker implantation.</p><p><strong>Methods: </strong>Retrospective analysis of patients implanted with the Perceval valve between 2007 and 2019 was performed by comparing patients implanted before the modification of sizing strategy (OLD group) and after (NEW group). The outcome parameters evaluated were the implanted prosthesis size, haemodynamical profile and postoperative pacemaker implantation.</p><p><strong>Results: </strong>The entire patient cohort (784 patients) consisted of 52% female patients, with a mean age of 78.53 [standard deviation (SD): 5.8] years and a mean EuroSCORE II of 6.3 (range 0.7-76). In 55.5% of cases, surgery was combined. The NEW cohort had more male patients (54.6% vs 43.4%) (P = 0.002). Mean implanted valve size, corrected for body surface area, was significantly lower in the NEW cohort (13.1, SD: 1.4 vs 13.5, SD: 1.4 mm/m2, P < 0.001). The 30-day mortality was 3.4%. Peak and mean transvalvular gradients at discharge were significantly lower in the NEW versus OLD groups: 24.4 mmHg (SD: 9.2) versus 28.4 mmHg (SD: 10.3) (P < 0.001) and 13.6 mmHg (SD: 5.3) versus 15.5 mmHg (SD: 6.0) (P < 0.001). The mean effective opening area and the indexed effective opening area, respectively, increased from 1.5 cm2 (SD: 0.5) and 0.85 cm2/m2 (SD: 0.27) in the OLD group to 1.7 cm2 (SD: 0.5) and 0.93 cm2/m2 (SD: 0.30) in the NEW group (P < 0.001). No difference was found in paravalvular leakage ≥1/4. Centrovalvular leakage ≥1/4 significantly decreased from 18% to 7.9% (P < 0.001). With the new sizing, the new postoperative pacemaker implantation rate decreased significantly from 11% to 6.1% (P = 0.016).</p><p><strong>Conclusions: </strong>Correct sizing of sutureless aortic valves is crucial to obtain the best possible haemodynamics and avoid complications.</p>","PeriodicalId":13621,"journal":{"name":"Interactive cardiovascular and thoracic surgery","volume":"35 2","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2022-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/11/0e/ivac157.PMC9272061.pdf","citationCount":"9","resultStr":"{\"title\":\"Avoiding oversizing in sutureless valves leads to lower transvalvular gradients and less permanent pacemaker implants postoperatively.\",\"authors\":\"Delphine Szecel, Marie Lamberigts, Filip Rega, Peter Verbrugghe, Christophe Dubois, Bart Meuris\",\"doi\":\"10.1093/icvts/ivac157\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>The aim of this study was to evaluate the impact of changing the sizing strategy in aortic valve replacement using the Perceval sutureless prosthesis on haemodynamic outcomes and postoperative pacemaker implantation.</p><p><strong>Methods: </strong>Retrospective analysis of patients implanted with the Perceval valve between 2007 and 2019 was performed by comparing patients implanted before the modification of sizing strategy (OLD group) and after (NEW group). The outcome parameters evaluated were the implanted prosthesis size, haemodynamical profile and postoperative pacemaker implantation.</p><p><strong>Results: </strong>The entire patient cohort (784 patients) consisted of 52% female patients, with a mean age of 78.53 [standard deviation (SD): 5.8] years and a mean EuroSCORE II of 6.3 (range 0.7-76). In 55.5% of cases, surgery was combined. The NEW cohort had more male patients (54.6% vs 43.4%) (P = 0.002). Mean implanted valve size, corrected for body surface area, was significantly lower in the NEW cohort (13.1, SD: 1.4 vs 13.5, SD: 1.4 mm/m2, P < 0.001). The 30-day mortality was 3.4%. Peak and mean transvalvular gradients at discharge were significantly lower in the NEW versus OLD groups: 24.4 mmHg (SD: 9.2) versus 28.4 mmHg (SD: 10.3) (P < 0.001) and 13.6 mmHg (SD: 5.3) versus 15.5 mmHg (SD: 6.0) (P < 0.001). The mean effective opening area and the indexed effective opening area, respectively, increased from 1.5 cm2 (SD: 0.5) and 0.85 cm2/m2 (SD: 0.27) in the OLD group to 1.7 cm2 (SD: 0.5) and 0.93 cm2/m2 (SD: 0.30) in the NEW group (P < 0.001). No difference was found in paravalvular leakage ≥1/4. Centrovalvular leakage ≥1/4 significantly decreased from 18% to 7.9% (P < 0.001). With the new sizing, the new postoperative pacemaker implantation rate decreased significantly from 11% to 6.1% (P = 0.016).</p><p><strong>Conclusions: </strong>Correct sizing of sutureless aortic valves is crucial to obtain the best possible haemodynamics and avoid complications.</p>\",\"PeriodicalId\":13621,\"journal\":{\"name\":\"Interactive cardiovascular and thoracic surgery\",\"volume\":\"35 2\",\"pages\":\"\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2022-07-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/11/0e/ivac157.PMC9272061.pdf\",\"citationCount\":\"9\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Interactive cardiovascular and thoracic surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/icvts/ivac157\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interactive cardiovascular and thoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/icvts/ivac157","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 9
摘要
目的:本研究的目的是评估使用Perceval无缝线假体主动脉瓣置换术中改变大小策略对血流动力学结果和术后起搏器植入的影响。方法:回顾性分析2007年至2019年植入Perceval瓣膜的患者,比较改变大小策略前(OLD组)和改变大小策略后(NEW组)植入的患者。评估的结果参数是植入假体的大小、血流动力学特征和术后起搏器植入。结果:整个患者队列(784例)中女性患者占52%,平均年龄78.53岁[标准差:5.8]岁,平均EuroSCORE II为6.3(范围0.7-76)。55.5%的病例联合手术。新队列中男性患者较多(54.6% vs 43.4%) (P = 0.002)。经体表面积校正后的平均植入瓣膜尺寸在NEW队列中显著降低(13.1,SD: 1.4 vs 13.5, SD: 1.4 mm/m2, P)。结论:正确的无缝线主动脉瓣尺寸对于获得最佳血流动力学和避免并发症至关重要。
Avoiding oversizing in sutureless valves leads to lower transvalvular gradients and less permanent pacemaker implants postoperatively.
Objectives: The aim of this study was to evaluate the impact of changing the sizing strategy in aortic valve replacement using the Perceval sutureless prosthesis on haemodynamic outcomes and postoperative pacemaker implantation.
Methods: Retrospective analysis of patients implanted with the Perceval valve between 2007 and 2019 was performed by comparing patients implanted before the modification of sizing strategy (OLD group) and after (NEW group). The outcome parameters evaluated were the implanted prosthesis size, haemodynamical profile and postoperative pacemaker implantation.
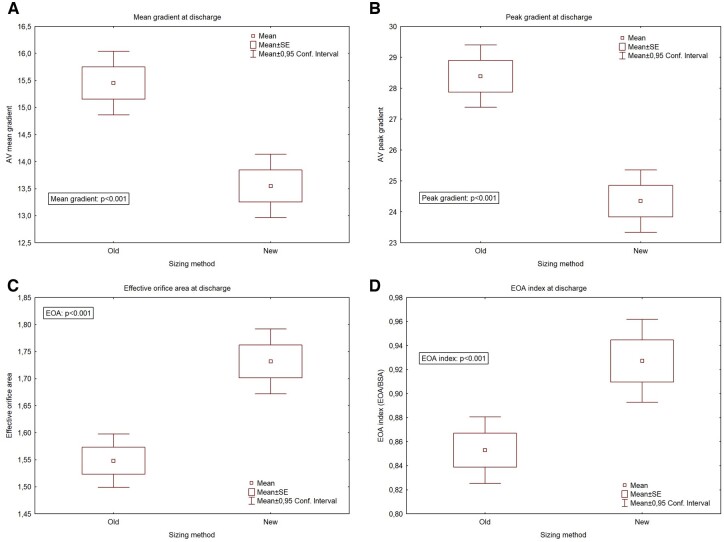
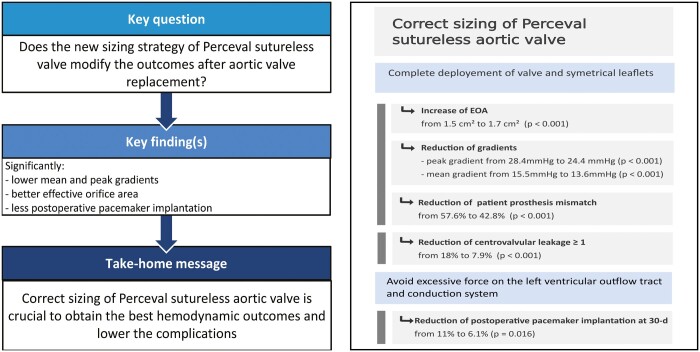
Results: The entire patient cohort (784 patients) consisted of 52% female patients, with a mean age of 78.53 [standard deviation (SD): 5.8] years and a mean EuroSCORE II of 6.3 (range 0.7-76). In 55.5% of cases, surgery was combined. The NEW cohort had more male patients (54.6% vs 43.4%) (P = 0.002). Mean implanted valve size, corrected for body surface area, was significantly lower in the NEW cohort (13.1, SD: 1.4 vs 13.5, SD: 1.4 mm/m2, P < 0.001). The 30-day mortality was 3.4%. Peak and mean transvalvular gradients at discharge were significantly lower in the NEW versus OLD groups: 24.4 mmHg (SD: 9.2) versus 28.4 mmHg (SD: 10.3) (P < 0.001) and 13.6 mmHg (SD: 5.3) versus 15.5 mmHg (SD: 6.0) (P < 0.001). The mean effective opening area and the indexed effective opening area, respectively, increased from 1.5 cm2 (SD: 0.5) and 0.85 cm2/m2 (SD: 0.27) in the OLD group to 1.7 cm2 (SD: 0.5) and 0.93 cm2/m2 (SD: 0.30) in the NEW group (P < 0.001). No difference was found in paravalvular leakage ≥1/4. Centrovalvular leakage ≥1/4 significantly decreased from 18% to 7.9% (P < 0.001). With the new sizing, the new postoperative pacemaker implantation rate decreased significantly from 11% to 6.1% (P = 0.016).
Conclusions: Correct sizing of sutureless aortic valves is crucial to obtain the best possible haemodynamics and avoid complications.
期刊介绍:
Interactive CardioVascular and Thoracic Surgery (ICVTS) publishes scientific contributions in the field of cardiovascular and thoracic surgery, covering all aspects of surgery of the heart, vessels and the chest. The journal publishes a range of article types including: Best Evidence Topics; Brief Communications; Case Reports; Original Articles; State-of-the-Art; Work in Progress Report.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
