{"title":"药物和内镜干预预防内镜后逆行胆管胰腺炎。","authors":"Emmanuel Palomera-Tejeda, Mihir Prakash Shah, Bashar M Attar, Hassam Shah, Bharosa Sharma, Roberto Oleas, Vikram Kotwal, Seema Gandhi, Hemant Raj Mutneja","doi":"10.14740/gr1620","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Post-endoscopic retrograde cholangiopancreatography pancreatitis (PEP) represents the most common serious complication after endoscopic retrograde cholangiopancreatography (ERCP). Rectal non-steroidal anti-inflammatory drugs (NSAIDs) and pancreatic duct stenting (PDS) are the prophylactic interventions with more evidence and efficacy; however, PEP still represents a significant source of morbidity, mortality, and economic burden. Chronic statin use has been proposed as a prophylactic method that could be cheap and relatively safe. However, the evidence is conflicting. We aimed to evaluate the impact of endoscopic and pharmacological interventions including chronic statin and aspirin use, on the development of PEP.</p><p><strong>Methods: </strong>A retrospective cohort study evaluated consecutive patients undergoing ERCP at John H. Stroger, Jr. Hospital of Cook County in Chicago from January 2015 to March 2018. Univariate and multivariate analyses were performed using logistic regression.</p><p><strong>Results: </strong>A total of 681 ERCPs were included in the study. Twelve (1.76%) developed PEP. Univariate, multivariate, and subgroup analyses did not show any association between chronic statin or aspirin use and PEP. PDS and rectal indomethacin were protective in patients undergoing pancreatic duct injection. Pancreatic duct injection, female sex, and younger age were associated with a higher risk. History of papillotomy was associated with lower risk only in the univariate analysis (all P values < 0.05).</p><p><strong>Conclusion: </strong>Chronic use of statins and aspirin appears to add no additional benefit to prevent ERCP pancreatitis. Rectal NSAIDs, and PDS after appropriate patient selection continue to be the main prophylactic measures. The lower incidence at our center compared with the reported data can be explained by the high rates of rectal indomethacin and PDS, the use of noninvasive diagnostic modalities for patient selection, and the expertise of the endoscopists.</p>","PeriodicalId":12461,"journal":{"name":"Gastroenterology Research","volume":"16 3","pages":"149-156"},"PeriodicalIF":1.7000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9b/90/gr-16-149.PMC10284647.pdf","citationCount":"0","resultStr":"{\"title\":\"Pharmacological and Endoscopic Interventions for Prophylaxis of Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis.\",\"authors\":\"Emmanuel Palomera-Tejeda, Mihir Prakash Shah, Bashar M Attar, Hassam Shah, Bharosa Sharma, Roberto Oleas, Vikram Kotwal, Seema Gandhi, Hemant Raj Mutneja\",\"doi\":\"10.14740/gr1620\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Post-endoscopic retrograde cholangiopancreatography pancreatitis (PEP) represents the most common serious complication after endoscopic retrograde cholangiopancreatography (ERCP). Rectal non-steroidal anti-inflammatory drugs (NSAIDs) and pancreatic duct stenting (PDS) are the prophylactic interventions with more evidence and efficacy; however, PEP still represents a significant source of morbidity, mortality, and economic burden. Chronic statin use has been proposed as a prophylactic method that could be cheap and relatively safe. However, the evidence is conflicting. We aimed to evaluate the impact of endoscopic and pharmacological interventions including chronic statin and aspirin use, on the development of PEP.</p><p><strong>Methods: </strong>A retrospective cohort study evaluated consecutive patients undergoing ERCP at John H. Stroger, Jr. Hospital of Cook County in Chicago from January 2015 to March 2018. Univariate and multivariate analyses were performed using logistic regression.</p><p><strong>Results: </strong>A total of 681 ERCPs were included in the study. Twelve (1.76%) developed PEP. Univariate, multivariate, and subgroup analyses did not show any association between chronic statin or aspirin use and PEP. PDS and rectal indomethacin were protective in patients undergoing pancreatic duct injection. Pancreatic duct injection, female sex, and younger age were associated with a higher risk. History of papillotomy was associated with lower risk only in the univariate analysis (all P values < 0.05).</p><p><strong>Conclusion: </strong>Chronic use of statins and aspirin appears to add no additional benefit to prevent ERCP pancreatitis. Rectal NSAIDs, and PDS after appropriate patient selection continue to be the main prophylactic measures. The lower incidence at our center compared with the reported data can be explained by the high rates of rectal indomethacin and PDS, the use of noninvasive diagnostic modalities for patient selection, and the expertise of the endoscopists.</p>\",\"PeriodicalId\":12461,\"journal\":{\"name\":\"Gastroenterology Research\",\"volume\":\"16 3\",\"pages\":\"149-156\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9b/90/gr-16-149.PMC10284647.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gastroenterology Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/gr1620\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastroenterology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/gr1620","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Pharmacological and Endoscopic Interventions for Prophylaxis of Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis.
Background: Post-endoscopic retrograde cholangiopancreatography pancreatitis (PEP) represents the most common serious complication after endoscopic retrograde cholangiopancreatography (ERCP). Rectal non-steroidal anti-inflammatory drugs (NSAIDs) and pancreatic duct stenting (PDS) are the prophylactic interventions with more evidence and efficacy; however, PEP still represents a significant source of morbidity, mortality, and economic burden. Chronic statin use has been proposed as a prophylactic method that could be cheap and relatively safe. However, the evidence is conflicting. We aimed to evaluate the impact of endoscopic and pharmacological interventions including chronic statin and aspirin use, on the development of PEP.
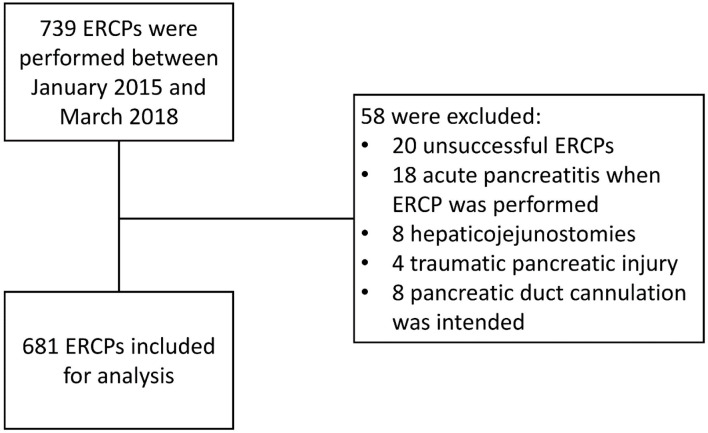
Methods: A retrospective cohort study evaluated consecutive patients undergoing ERCP at John H. Stroger, Jr. Hospital of Cook County in Chicago from January 2015 to March 2018. Univariate and multivariate analyses were performed using logistic regression.
Results: A total of 681 ERCPs were included in the study. Twelve (1.76%) developed PEP. Univariate, multivariate, and subgroup analyses did not show any association between chronic statin or aspirin use and PEP. PDS and rectal indomethacin were protective in patients undergoing pancreatic duct injection. Pancreatic duct injection, female sex, and younger age were associated with a higher risk. History of papillotomy was associated with lower risk only in the univariate analysis (all P values < 0.05).
Conclusion: Chronic use of statins and aspirin appears to add no additional benefit to prevent ERCP pancreatitis. Rectal NSAIDs, and PDS after appropriate patient selection continue to be the main prophylactic measures. The lower incidence at our center compared with the reported data can be explained by the high rates of rectal indomethacin and PDS, the use of noninvasive diagnostic modalities for patient selection, and the expertise of the endoscopists.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
