{"title":"右胸内动脉与右胃网膜动脉复合移植在冠状动脉搭桥术中的应用。","authors":"Makoto Shirakawa, Masami Ochi, Yosuke Ishii","doi":"10.5761/atcs.oa.22-00171","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>When added to the internal thoracic artery (ITA), the right gastroepiploic artery (GEA) has been used as an in-situ graft or an I-composite right ITA-right GEA graft in coronary artery bypass grafting (CABG). We aimed to verify its potential.</p><p><strong>Methods: </strong>We evaluated 104 patients who underwent first isolated CABG with this I-composite graft. The number of distal anastomoses, graft flow (GF) and pulsatility index (PI) during surgery, and graft patency in the early term regarding this I-composite graft were evaluated.</p><p><strong>Results: </strong>The number of total distal anastomoses and distal anastomoses with arterial grafts were 4.17 ± 0.81 and 3.63 ± 0.81, respectively. This I-composite graft achieved 2.38 ± 0.69 distal anastomoses. GF tended to increase according to the increased number of distal anastomoses (p = 0.241), and the PI maintained a low score regardless of the number of distal anastomoses (p = 0.834). Graft patency was 95.5%; moreover, the number of distal anastomoses with this I-composite graft did not affect early-term graft patency.</p><p><strong>Conclusion: </strong>Right GEA utility was expanded as this I-composite graft in addition to in-situ graft. This I-composite graft has an adequate flow capacity for revascularization in non-left anterior descending coronary artery lesions.</p>","PeriodicalId":8037,"journal":{"name":"Annals of Thoracic and Cardiovascular Surgery","volume":"29 2","pages":"86-92"},"PeriodicalIF":1.3000,"publicationDate":"2023-04-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6d/9c/atcs-29-086.PMC10126763.pdf","citationCount":"1","resultStr":"{\"title\":\"I-Composite Graft with Right Internal Thoracic Artery and Right Gastroepiploic Artery in Coronary Artery Bypass Grafting.\",\"authors\":\"Makoto Shirakawa, Masami Ochi, Yosuke Ishii\",\"doi\":\"10.5761/atcs.oa.22-00171\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>When added to the internal thoracic artery (ITA), the right gastroepiploic artery (GEA) has been used as an in-situ graft or an I-composite right ITA-right GEA graft in coronary artery bypass grafting (CABG). We aimed to verify its potential.</p><p><strong>Methods: </strong>We evaluated 104 patients who underwent first isolated CABG with this I-composite graft. The number of distal anastomoses, graft flow (GF) and pulsatility index (PI) during surgery, and graft patency in the early term regarding this I-composite graft were evaluated.</p><p><strong>Results: </strong>The number of total distal anastomoses and distal anastomoses with arterial grafts were 4.17 ± 0.81 and 3.63 ± 0.81, respectively. This I-composite graft achieved 2.38 ± 0.69 distal anastomoses. GF tended to increase according to the increased number of distal anastomoses (p = 0.241), and the PI maintained a low score regardless of the number of distal anastomoses (p = 0.834). Graft patency was 95.5%; moreover, the number of distal anastomoses with this I-composite graft did not affect early-term graft patency.</p><p><strong>Conclusion: </strong>Right GEA utility was expanded as this I-composite graft in addition to in-situ graft. This I-composite graft has an adequate flow capacity for revascularization in non-left anterior descending coronary artery lesions.</p>\",\"PeriodicalId\":8037,\"journal\":{\"name\":\"Annals of Thoracic and Cardiovascular Surgery\",\"volume\":\"29 2\",\"pages\":\"86-92\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2023-04-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6d/9c/atcs-29-086.PMC10126763.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5761/atcs.oa.22-00171\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5761/atcs.oa.22-00171","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
I-Composite Graft with Right Internal Thoracic Artery and Right Gastroepiploic Artery in Coronary Artery Bypass Grafting.
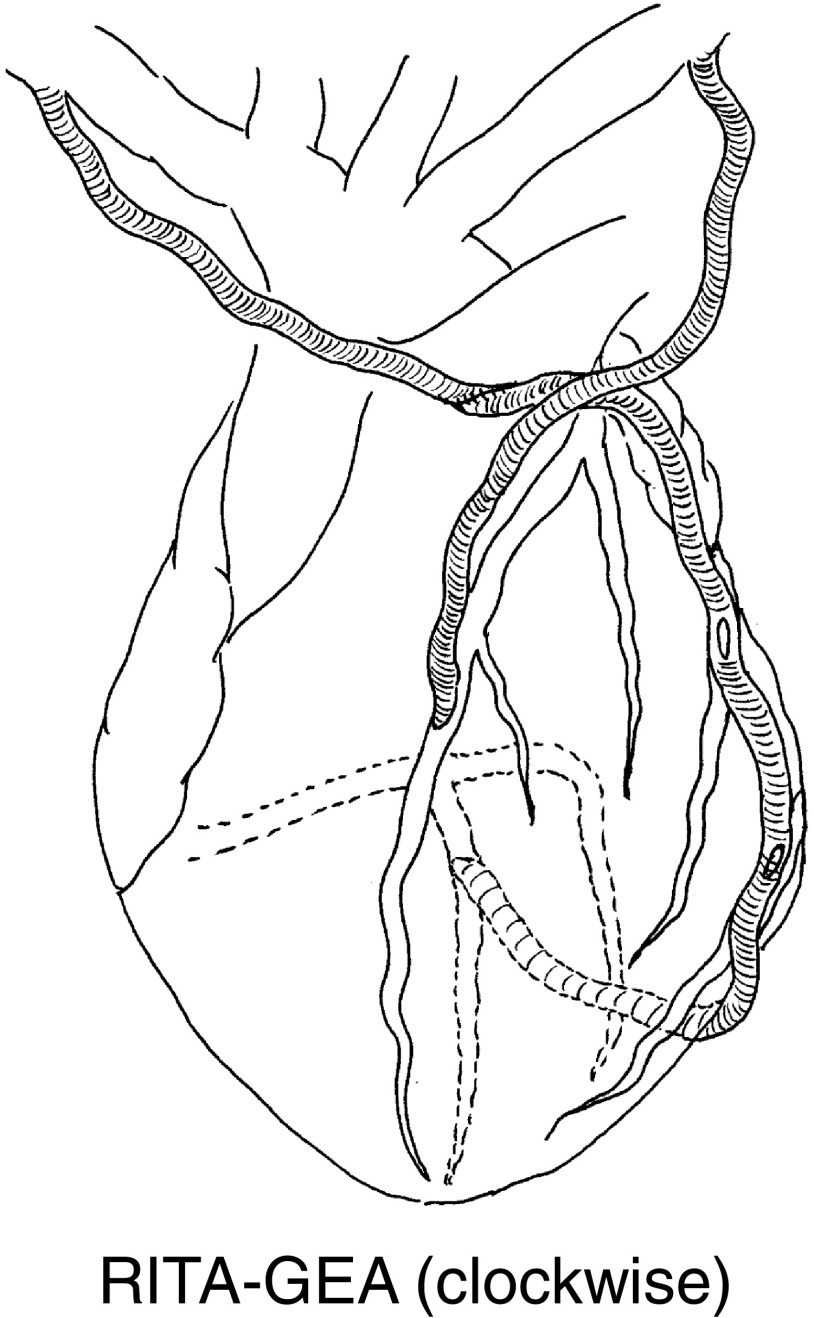
Purpose: When added to the internal thoracic artery (ITA), the right gastroepiploic artery (GEA) has been used as an in-situ graft or an I-composite right ITA-right GEA graft in coronary artery bypass grafting (CABG). We aimed to verify its potential.
Methods: We evaluated 104 patients who underwent first isolated CABG with this I-composite graft. The number of distal anastomoses, graft flow (GF) and pulsatility index (PI) during surgery, and graft patency in the early term regarding this I-composite graft were evaluated.
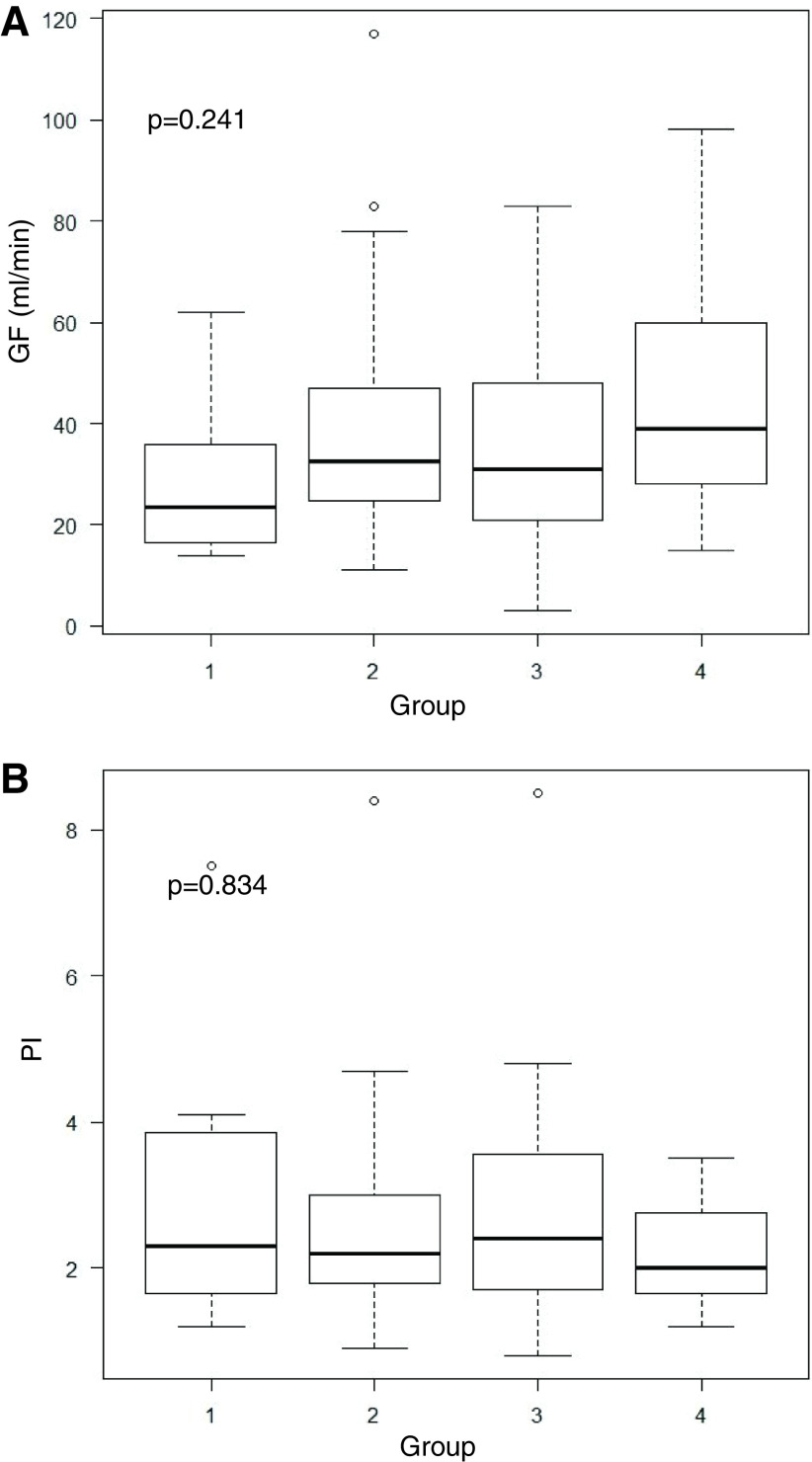
Results: The number of total distal anastomoses and distal anastomoses with arterial grafts were 4.17 ± 0.81 and 3.63 ± 0.81, respectively. This I-composite graft achieved 2.38 ± 0.69 distal anastomoses. GF tended to increase according to the increased number of distal anastomoses (p = 0.241), and the PI maintained a low score regardless of the number of distal anastomoses (p = 0.834). Graft patency was 95.5%; moreover, the number of distal anastomoses with this I-composite graft did not affect early-term graft patency.
Conclusion: Right GEA utility was expanded as this I-composite graft in addition to in-situ graft. This I-composite graft has an adequate flow capacity for revascularization in non-left anterior descending coronary artery lesions.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
