Gerard M Walls, Michael McMahon, Natasha Moore, Patrick Nicol, Gemma Bradley, Glenn Whitten, Linda Young, Jolyne M O'Hare, John Lindsay, Ryan Connolly, Dermot Linden, Peter A Ball, Gerard G Hanna, Jonathan McAleese
{"title":"间质性肺病患者癌症根治性放疗后的临床病理结果。","authors":"Gerard M Walls, Michael McMahon, Natasha Moore, Patrick Nicol, Gemma Bradley, Glenn Whitten, Linda Young, Jolyne M O'Hare, John Lindsay, Ryan Connolly, Dermot Linden, Peter A Ball, Gerard G Hanna, Jonathan McAleese","doi":"10.1259/bjro.20220049","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Interstitial lung disease (ILD) is relatively common in patients with lung cancer with an incidence of 7.5%. Historically pre-existing ILD was a contraindication to radical radiotherapy owing to increased radiation pneumonitis rates, worsened fibrosis and poorer survival compared with non-ILD cohorts. Herein, the clinical and radiological toxicity outcomes of a contemporaneous cohort are described.</p><p><strong>Methods: </strong>Patients with ILD treated with radical radiotherapy for lung cancer at a regional cancer centre were collected prospectively. Radiotherapy planning, tumour characteristics, and pre- and post-treatment functional and radiological parameters were recorded. Cross-sectional images were independently assessed by two Consultant Thoracic Radiologists.</p><p><strong>Results: </strong>Twenty-seven patients with co-existing ILD received radical radiotherapy from February 2009 to April 2019, with predominance of usual interstitial pneumonia subtype (52%). According to ILD-GAP scores, most patients were Stage I. After radiotherapy, localised (41%) or extensive (41%) progressive interstitial changes were noted for most patients yet dyspnoea scores (<i>n</i> = 15 available) and spirometry (<i>n</i> = 10 available) were stable. One-third of patients with ILD went on to receive long-term oxygen therapy, which was significantly more than the non-ILD cohort. Median survival trended towards being worse compared with non-ILD cases (17.8 <i>vs</i> 24.0 months, <i>p</i> = 0.834).</p><p><strong>Conclusion: </strong>Radiological progression of ILD and reduced survival were observed post-radiotherapy in this small cohort receiving lung cancer radiotherapy, although a matched functional decline was frequently absent. Although there is an excess of early deaths, long-term disease control is achievable.</p><p><strong>Advances in knowledge: </strong>For selected patients with ILD, long-term lung cancer control without severely impacting respiratory function may be possible with radical radiotherapy, albeit with a slightly higher risk of death.</p>","PeriodicalId":72419,"journal":{"name":"BJR open","volume":"5 1","pages":"20220049"},"PeriodicalIF":2.1000,"publicationDate":"2023-04-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10301718/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinicoradiological outcomes after radical radiotherapy for lung cancer in patients with interstitial lung disease.\",\"authors\":\"Gerard M Walls, Michael McMahon, Natasha Moore, Patrick Nicol, Gemma Bradley, Glenn Whitten, Linda Young, Jolyne M O'Hare, John Lindsay, Ryan Connolly, Dermot Linden, Peter A Ball, Gerard G Hanna, Jonathan McAleese\",\"doi\":\"10.1259/bjro.20220049\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Interstitial lung disease (ILD) is relatively common in patients with lung cancer with an incidence of 7.5%. Historically pre-existing ILD was a contraindication to radical radiotherapy owing to increased radiation pneumonitis rates, worsened fibrosis and poorer survival compared with non-ILD cohorts. Herein, the clinical and radiological toxicity outcomes of a contemporaneous cohort are described.</p><p><strong>Methods: </strong>Patients with ILD treated with radical radiotherapy for lung cancer at a regional cancer centre were collected prospectively. Radiotherapy planning, tumour characteristics, and pre- and post-treatment functional and radiological parameters were recorded. Cross-sectional images were independently assessed by two Consultant Thoracic Radiologists.</p><p><strong>Results: </strong>Twenty-seven patients with co-existing ILD received radical radiotherapy from February 2009 to April 2019, with predominance of usual interstitial pneumonia subtype (52%). According to ILD-GAP scores, most patients were Stage I. After radiotherapy, localised (41%) or extensive (41%) progressive interstitial changes were noted for most patients yet dyspnoea scores (<i>n</i> = 15 available) and spirometry (<i>n</i> = 10 available) were stable. One-third of patients with ILD went on to receive long-term oxygen therapy, which was significantly more than the non-ILD cohort. Median survival trended towards being worse compared with non-ILD cases (17.8 <i>vs</i> 24.0 months, <i>p</i> = 0.834).</p><p><strong>Conclusion: </strong>Radiological progression of ILD and reduced survival were observed post-radiotherapy in this small cohort receiving lung cancer radiotherapy, although a matched functional decline was frequently absent. Although there is an excess of early deaths, long-term disease control is achievable.</p><p><strong>Advances in knowledge: </strong>For selected patients with ILD, long-term lung cancer control without severely impacting respiratory function may be possible with radical radiotherapy, albeit with a slightly higher risk of death.</p>\",\"PeriodicalId\":72419,\"journal\":{\"name\":\"BJR open\",\"volume\":\"5 1\",\"pages\":\"20220049\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-04-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10301718/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BJR open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1259/bjro.20220049\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJR open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1259/bjro.20220049","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Clinicoradiological outcomes after radical radiotherapy for lung cancer in patients with interstitial lung disease.
Objective: Interstitial lung disease (ILD) is relatively common in patients with lung cancer with an incidence of 7.5%. Historically pre-existing ILD was a contraindication to radical radiotherapy owing to increased radiation pneumonitis rates, worsened fibrosis and poorer survival compared with non-ILD cohorts. Herein, the clinical and radiological toxicity outcomes of a contemporaneous cohort are described.
Methods: Patients with ILD treated with radical radiotherapy for lung cancer at a regional cancer centre were collected prospectively. Radiotherapy planning, tumour characteristics, and pre- and post-treatment functional and radiological parameters were recorded. Cross-sectional images were independently assessed by two Consultant Thoracic Radiologists.
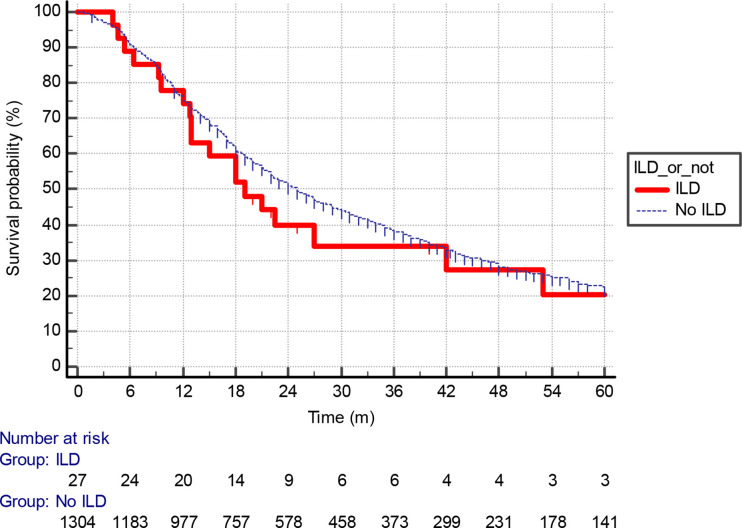
Results: Twenty-seven patients with co-existing ILD received radical radiotherapy from February 2009 to April 2019, with predominance of usual interstitial pneumonia subtype (52%). According to ILD-GAP scores, most patients were Stage I. After radiotherapy, localised (41%) or extensive (41%) progressive interstitial changes were noted for most patients yet dyspnoea scores (n = 15 available) and spirometry (n = 10 available) were stable. One-third of patients with ILD went on to receive long-term oxygen therapy, which was significantly more than the non-ILD cohort. Median survival trended towards being worse compared with non-ILD cases (17.8 vs 24.0 months, p = 0.834).
Conclusion: Radiological progression of ILD and reduced survival were observed post-radiotherapy in this small cohort receiving lung cancer radiotherapy, although a matched functional decline was frequently absent. Although there is an excess of early deaths, long-term disease control is achievable.
Advances in knowledge: For selected patients with ILD, long-term lung cancer control without severely impacting respiratory function may be possible with radical radiotherapy, albeit with a slightly higher risk of death.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
