Sabrina Terrizzi , A. Lanethea Mathews-Schultz , Michele Moser Deegan
{"title":"州与联邦医疗保险市场:医疗补助大了,个人强制医保小了","authors":"Sabrina Terrizzi , A. Lanethea Mathews-Schultz , Michele Moser Deegan","doi":"10.1016/j.hpopen.2021.100059","DOIUrl":null,"url":null,"abstract":"<div><p>States retain significant power over key components of Affordable Care Act implementation. Using data from the US Census from 2010 to 2018, we examine how states’ decisions to either establish state-run marketplaces or to default to the federal marketplace influenced the distribution of health insurance types within states. We find, somewhat counterintuitively, that state-based marketplaces are associated with greater change in enrollment for Medicaid compared to the federal marketplace. These findings confirm that, at least until 2018, the most significant increases in insurance coverage resulting from the ACA were in public insurance, rather than private insurance. We explore a number of possible explanations to help explain these findings, raising important questions about the efficacy of the individual mandate (a key mechanism in legislative efforts to reduce the numbers of uninsured), the related administrative burdens associated with state and federal marketplaces, and, equally as important, differential access to Medicaid entitlements among citizens living in different states—access that hinges not only or always on Medicaid expansion, but also and perhaps more importantly, on policy decisions about insurance marketplaces.</p></div>","PeriodicalId":34527,"journal":{"name":"Health Policy Open","volume":"3 ","pages":"Article 100059"},"PeriodicalIF":2.3000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3b/4b/main.PMC10297752.pdf","citationCount":"1","resultStr":"{\"title\":\"State versus federal health insurance marketplaces: A bigger deal for Medicaid and a smaller deal for the individual mandate\",\"authors\":\"Sabrina Terrizzi , A. Lanethea Mathews-Schultz , Michele Moser Deegan\",\"doi\":\"10.1016/j.hpopen.2021.100059\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p>States retain significant power over key components of Affordable Care Act implementation. Using data from the US Census from 2010 to 2018, we examine how states’ decisions to either establish state-run marketplaces or to default to the federal marketplace influenced the distribution of health insurance types within states. We find, somewhat counterintuitively, that state-based marketplaces are associated with greater change in enrollment for Medicaid compared to the federal marketplace. These findings confirm that, at least until 2018, the most significant increases in insurance coverage resulting from the ACA were in public insurance, rather than private insurance. We explore a number of possible explanations to help explain these findings, raising important questions about the efficacy of the individual mandate (a key mechanism in legislative efforts to reduce the numbers of uninsured), the related administrative burdens associated with state and federal marketplaces, and, equally as important, differential access to Medicaid entitlements among citizens living in different states—access that hinges not only or always on Medicaid expansion, but also and perhaps more importantly, on policy decisions about insurance marketplaces.</p></div>\",\"PeriodicalId\":34527,\"journal\":{\"name\":\"Health Policy Open\",\"volume\":\"3 \",\"pages\":\"Article 100059\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3b/4b/main.PMC10297752.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Health Policy Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2590229621000307\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/12/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Policy Open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590229621000307","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/12/2 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
State versus federal health insurance marketplaces: A bigger deal for Medicaid and a smaller deal for the individual mandate
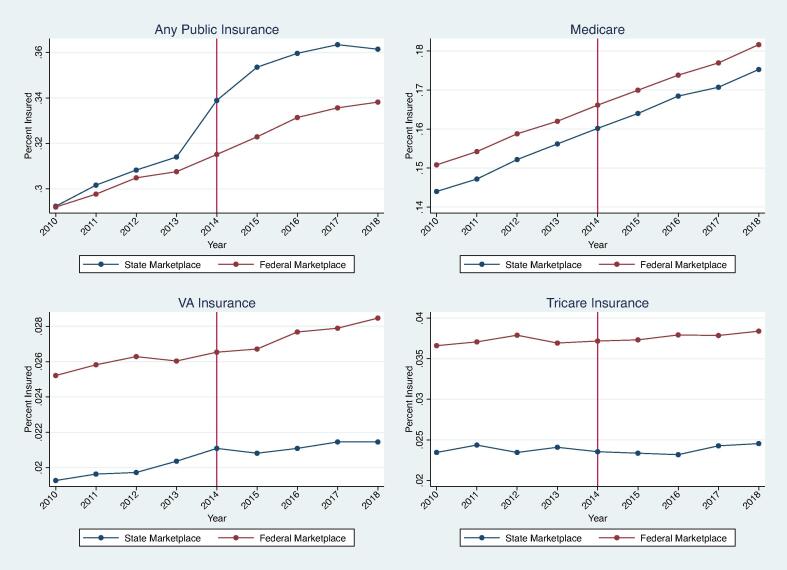
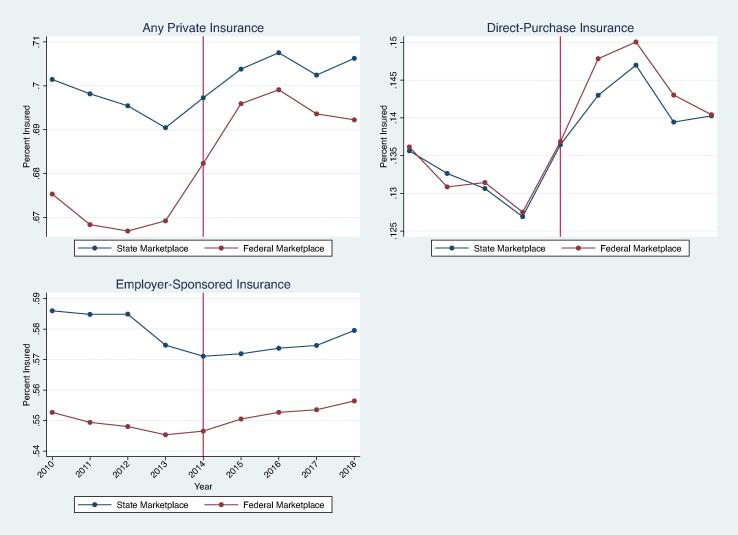
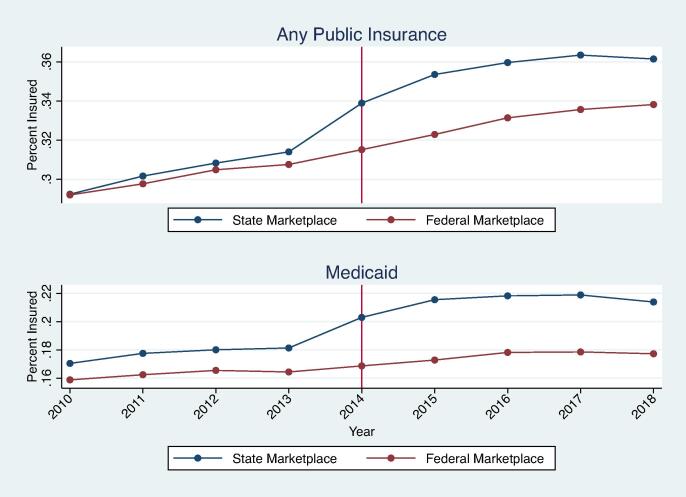
States retain significant power over key components of Affordable Care Act implementation. Using data from the US Census from 2010 to 2018, we examine how states’ decisions to either establish state-run marketplaces or to default to the federal marketplace influenced the distribution of health insurance types within states. We find, somewhat counterintuitively, that state-based marketplaces are associated with greater change in enrollment for Medicaid compared to the federal marketplace. These findings confirm that, at least until 2018, the most significant increases in insurance coverage resulting from the ACA were in public insurance, rather than private insurance. We explore a number of possible explanations to help explain these findings, raising important questions about the efficacy of the individual mandate (a key mechanism in legislative efforts to reduce the numbers of uninsured), the related administrative burdens associated with state and federal marketplaces, and, equally as important, differential access to Medicaid entitlements among citizens living in different states—access that hinges not only or always on Medicaid expansion, but also and perhaps more importantly, on policy decisions about insurance marketplaces.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
