{"title":"缺血性心肌病的心源性猝死和一级预防:是时候采取更个性化的方法了?","authors":"Saad M Ezad, Girish Babu, Peter O'Kane","doi":"10.15420/icr.2022.14","DOIUrl":null,"url":null,"abstract":"<p><p>Guidelines recommend primary prevention implantable cardioverter defibrillator (PPICD) for left ventricular ejection fraction (LVEF) <35% only after 3 months of optimal medical therapy (OMT) or 6 weeks after acute MI with persistent LVEF dysfunction. A 73-year-old woman presented with decompensated heart failure secondary to ischaemic cardiomyopathy. Severe coronary disease with sufficient dysfunctional myocardial segments on cardiac MRI suggested potential benefit from revascularisation. Following discussion with the heart team, she underwent percutaneous coronary intervention (PCI). PPICD implantation was deferred as per guideline recommendations. However, 20 days post-PCI, the patient died from malignant ventricular arrhythmia captured on a Holter monitor. This case demonstrates that some high-risk patients may not receive a potentially life-saving PPICD if guidelines are stringently adhered to. We highlight evidence that LVEF alone is of limited value in a risk assessment of arrhythmogenic death, and postulate that a more personalised ICD prescription should be considered using scar characteristics on cardiac MRI to prompt upstream ICD implantation in high-risk patients.</p>","PeriodicalId":38586,"journal":{"name":"Interventional Cardiology Review","volume":"18 ","pages":"e11"},"PeriodicalIF":2.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/12/c6/icr-18-e11.PMC10311393.pdf","citationCount":"0","resultStr":"{\"title\":\"Sudden Cardiac Death in Ischaemic Cardiomyopathy and the Primary Prevention ICD: Time for a More a Personalised Approach?\",\"authors\":\"Saad M Ezad, Girish Babu, Peter O'Kane\",\"doi\":\"10.15420/icr.2022.14\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Guidelines recommend primary prevention implantable cardioverter defibrillator (PPICD) for left ventricular ejection fraction (LVEF) <35% only after 3 months of optimal medical therapy (OMT) or 6 weeks after acute MI with persistent LVEF dysfunction. A 73-year-old woman presented with decompensated heart failure secondary to ischaemic cardiomyopathy. Severe coronary disease with sufficient dysfunctional myocardial segments on cardiac MRI suggested potential benefit from revascularisation. Following discussion with the heart team, she underwent percutaneous coronary intervention (PCI). PPICD implantation was deferred as per guideline recommendations. However, 20 days post-PCI, the patient died from malignant ventricular arrhythmia captured on a Holter monitor. This case demonstrates that some high-risk patients may not receive a potentially life-saving PPICD if guidelines are stringently adhered to. We highlight evidence that LVEF alone is of limited value in a risk assessment of arrhythmogenic death, and postulate that a more personalised ICD prescription should be considered using scar characteristics on cardiac MRI to prompt upstream ICD implantation in high-risk patients.</p>\",\"PeriodicalId\":38586,\"journal\":{\"name\":\"Interventional Cardiology Review\",\"volume\":\"18 \",\"pages\":\"e11\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/12/c6/icr-18-e11.PMC10311393.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Interventional Cardiology Review\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.15420/icr.2022.14\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"0\",\"JCRName\":\"PHILOSOPHY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interventional Cardiology Review","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15420/icr.2022.14","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"PHILOSOPHY","Score":null,"Total":0}
Sudden Cardiac Death in Ischaemic Cardiomyopathy and the Primary Prevention ICD: Time for a More a Personalised Approach?
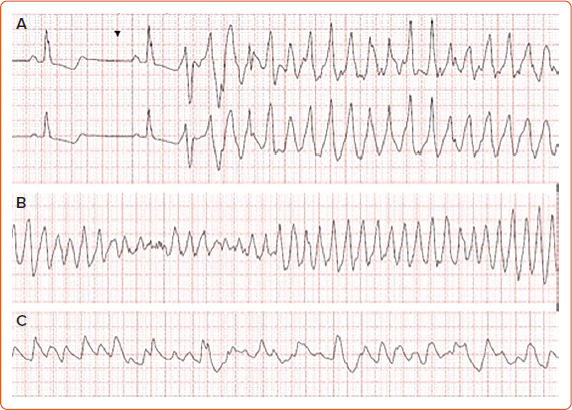
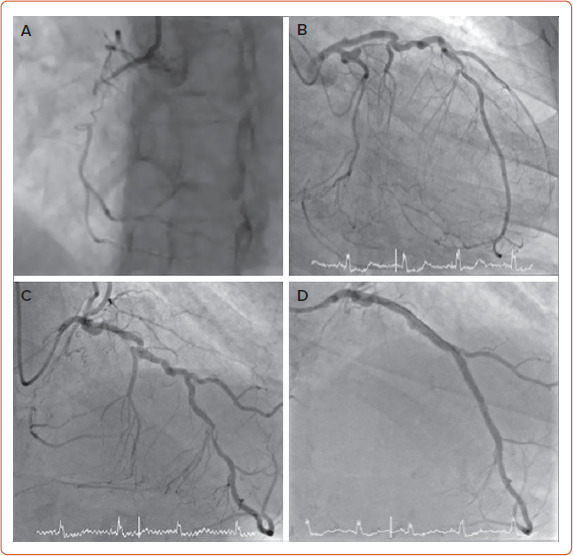
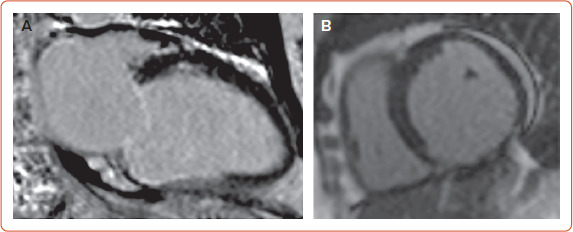
Guidelines recommend primary prevention implantable cardioverter defibrillator (PPICD) for left ventricular ejection fraction (LVEF) <35% only after 3 months of optimal medical therapy (OMT) or 6 weeks after acute MI with persistent LVEF dysfunction. A 73-year-old woman presented with decompensated heart failure secondary to ischaemic cardiomyopathy. Severe coronary disease with sufficient dysfunctional myocardial segments on cardiac MRI suggested potential benefit from revascularisation. Following discussion with the heart team, she underwent percutaneous coronary intervention (PCI). PPICD implantation was deferred as per guideline recommendations. However, 20 days post-PCI, the patient died from malignant ventricular arrhythmia captured on a Holter monitor. This case demonstrates that some high-risk patients may not receive a potentially life-saving PPICD if guidelines are stringently adhered to. We highlight evidence that LVEF alone is of limited value in a risk assessment of arrhythmogenic death, and postulate that a more personalised ICD prescription should be considered using scar characteristics on cardiac MRI to prompt upstream ICD implantation in high-risk patients.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
