{"title":"尿酸转运蛋白1与其他尿酸转运蛋白的微妙串扰在多替努拉德诱导的慢性肾病和心血管疾病中可能存在。","authors":"Hidekatsu Yanai, Hiroki Adachi, Mariko Hakoshima, Hisayuki Katsuyama","doi":"10.14740/cr1496","DOIUrl":null,"url":null,"abstract":"We previously reported that the switching from fenofibrate to the selective peroxisome proliferator-activated receptor (PPAR) α modulator, pemafibrate, increased serum uric acid (UA) levels and reduced estimated glomerular filtration rate (eGFR) in patients with dyslipidemia [1]. Fenofibrate has a property to decrease serum UA by inhibition of urate transporter 1 (URAT1) by its major metabolite [2]. Although fenofibrate was reported to decrease the eGFR [3], the mechanism of fenofibrate-induced renal impairment has been remained unclear. Further, our previous discussion on such issue was premature [1]. Recently, the role of UA transporters has been clarified [4] (Fig. 1a). Renal excretion of UA is the major regulator of serum UA, and renal UA reabsorption is mainly mediated by URAT1 and glucose transporter 9 (GLUT9). Organic anion transporters (OATs) 1, 3 transport UA from the renal interstitial into renal proximal tubule epithelial cells. ATP-binding cassette, subfamily G, 2 (ABCG2) has been identified as a high-capacity UA exporter that mediates renal and/or extrarenal UA excretion. Indoxyl sulfate (IS) is a well-known uremic toxin that accumulates under renal impairment and is involved in the progression of chronic kidney disease (CKD) and cardiovascular disease (CVD), by inducing inflammation and free radical production [5, 6]. IS excretion is also mediated by OAT1/3 and ABCG2 as well as UA excretion [4]. ABCG2 inhibitors, such as febuxostat (xanthin oxidase (XO) inhibitor), caused renal IS accumulation by suppressing its excretion via ABCG2 in rats [7]. Fenofibrate completely inhibits ABCG2 which may lead to increase in renal IS [8], resulting in elevation of eGFR. Another XO inhibitor, topiroxostat, also inhibits ABCG2, however, allopurinol does not inhibit ABCG2. OAT inhibitors such as probenecid (uricosuric drug, URAT1, and GLUT9 inhibitor), suppressed IS uptake into the kidney, leading to increased plasma IS [7]. Increased plasma IS may be harmful to cardiovascular system by inducing inflammation and free radical production. Benzbromarone (uricosuric drug) inhibits OAT1 and OAT3, however, its inhibitory potency for OAT1/3 is lower than those of probenecid [9], which may not lead to an increase in plasma IS. Probenecid and benzbromarone inhibit ABCG2, which may be unfavorably associated with renal function. In short, the inhibition of OAT1/3 and ABCG2 increase IS in plasma and kidney, which may be unfavorably associated with the development of CVD and CKD, respectively. Very recently, we reported that the addition of the selective URAT1 inhibitor dotinurad to highly-evidence-proved drugs to improve CKD such as sodium-glucose cotransporter 2 (SGLT2) inhibitor and a glucagon-like peptide 1 (GLP-1) receptor agonist, improved eGFR in a diabetic patient with CKD stage G4 [10]. Dotinurad inhibits URAT1 specifically, however, does not inhibit ABCG2 [9], and reduces renal UA accumulation, which may increase the transport of renal accumulated IS by ABCG2 because UA may compete with IS for ABCG2 (Fig. 1b). This exquisite crosstalk between URAT1 and ABCG2 induced by dotinurad may be beneficially associated with the development and progression of CKD. Our recent study showed that dotinurad reduced urinary albumin creatinine ratio (UACR) and increased eGFR in patients with CKD [11], supporting our hypothesis. Dotinurad does not inhibit OAT1/3, and then does not increase plasma IS [7]. Possibly, plasma IS may decrease when renal IS decreased because renal excretion is the major regulator of blood UA and IS. This excellent crosstalk between URAT1 and OAT1/3 induced by dotinurad may be favorably associated with the development of CVD. In conclusion, the selective inhibition of URAT1 by dotinurad may induce favorable metabolic changes of uremic toxin, which may be beneficially associated with the development and progression of CKD and CVD.","PeriodicalId":9424,"journal":{"name":"Cardiology Research","volume":"14 2","pages":"158-160"},"PeriodicalIF":1.4000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e1/15/cr-14-158.PMC10116931.pdf","citationCount":"0","resultStr":"{\"title\":\"A Possible Exquisite Crosstalk of Urate Transporter 1 With Other Urate Transporters for Chronic Kidney Disease and Cardiovascular Disease Induced by Dotinurad.\",\"authors\":\"Hidekatsu Yanai, Hiroki Adachi, Mariko Hakoshima, Hisayuki Katsuyama\",\"doi\":\"10.14740/cr1496\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"We previously reported that the switching from fenofibrate to the selective peroxisome proliferator-activated receptor (PPAR) α modulator, pemafibrate, increased serum uric acid (UA) levels and reduced estimated glomerular filtration rate (eGFR) in patients with dyslipidemia [1]. Fenofibrate has a property to decrease serum UA by inhibition of urate transporter 1 (URAT1) by its major metabolite [2]. Although fenofibrate was reported to decrease the eGFR [3], the mechanism of fenofibrate-induced renal impairment has been remained unclear. Further, our previous discussion on such issue was premature [1]. Recently, the role of UA transporters has been clarified [4] (Fig. 1a). Renal excretion of UA is the major regulator of serum UA, and renal UA reabsorption is mainly mediated by URAT1 and glucose transporter 9 (GLUT9). Organic anion transporters (OATs) 1, 3 transport UA from the renal interstitial into renal proximal tubule epithelial cells. ATP-binding cassette, subfamily G, 2 (ABCG2) has been identified as a high-capacity UA exporter that mediates renal and/or extrarenal UA excretion. Indoxyl sulfate (IS) is a well-known uremic toxin that accumulates under renal impairment and is involved in the progression of chronic kidney disease (CKD) and cardiovascular disease (CVD), by inducing inflammation and free radical production [5, 6]. IS excretion is also mediated by OAT1/3 and ABCG2 as well as UA excretion [4]. ABCG2 inhibitors, such as febuxostat (xanthin oxidase (XO) inhibitor), caused renal IS accumulation by suppressing its excretion via ABCG2 in rats [7]. Fenofibrate completely inhibits ABCG2 which may lead to increase in renal IS [8], resulting in elevation of eGFR. Another XO inhibitor, topiroxostat, also inhibits ABCG2, however, allopurinol does not inhibit ABCG2. OAT inhibitors such as probenecid (uricosuric drug, URAT1, and GLUT9 inhibitor), suppressed IS uptake into the kidney, leading to increased plasma IS [7]. Increased plasma IS may be harmful to cardiovascular system by inducing inflammation and free radical production. Benzbromarone (uricosuric drug) inhibits OAT1 and OAT3, however, its inhibitory potency for OAT1/3 is lower than those of probenecid [9], which may not lead to an increase in plasma IS. Probenecid and benzbromarone inhibit ABCG2, which may be unfavorably associated with renal function. In short, the inhibition of OAT1/3 and ABCG2 increase IS in plasma and kidney, which may be unfavorably associated with the development of CVD and CKD, respectively. Very recently, we reported that the addition of the selective URAT1 inhibitor dotinurad to highly-evidence-proved drugs to improve CKD such as sodium-glucose cotransporter 2 (SGLT2) inhibitor and a glucagon-like peptide 1 (GLP-1) receptor agonist, improved eGFR in a diabetic patient with CKD stage G4 [10]. Dotinurad inhibits URAT1 specifically, however, does not inhibit ABCG2 [9], and reduces renal UA accumulation, which may increase the transport of renal accumulated IS by ABCG2 because UA may compete with IS for ABCG2 (Fig. 1b). This exquisite crosstalk between URAT1 and ABCG2 induced by dotinurad may be beneficially associated with the development and progression of CKD. Our recent study showed that dotinurad reduced urinary albumin creatinine ratio (UACR) and increased eGFR in patients with CKD [11], supporting our hypothesis. Dotinurad does not inhibit OAT1/3, and then does not increase plasma IS [7]. Possibly, plasma IS may decrease when renal IS decreased because renal excretion is the major regulator of blood UA and IS. This excellent crosstalk between URAT1 and OAT1/3 induced by dotinurad may be favorably associated with the development of CVD. In conclusion, the selective inhibition of URAT1 by dotinurad may induce favorable metabolic changes of uremic toxin, which may be beneficially associated with the development and progression of CKD and CVD.\",\"PeriodicalId\":9424,\"journal\":{\"name\":\"Cardiology Research\",\"volume\":\"14 2\",\"pages\":\"158-160\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e1/15/cr-14-158.PMC10116931.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/cr1496\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/cr1496","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
A Possible Exquisite Crosstalk of Urate Transporter 1 With Other Urate Transporters for Chronic Kidney Disease and Cardiovascular Disease Induced by Dotinurad.
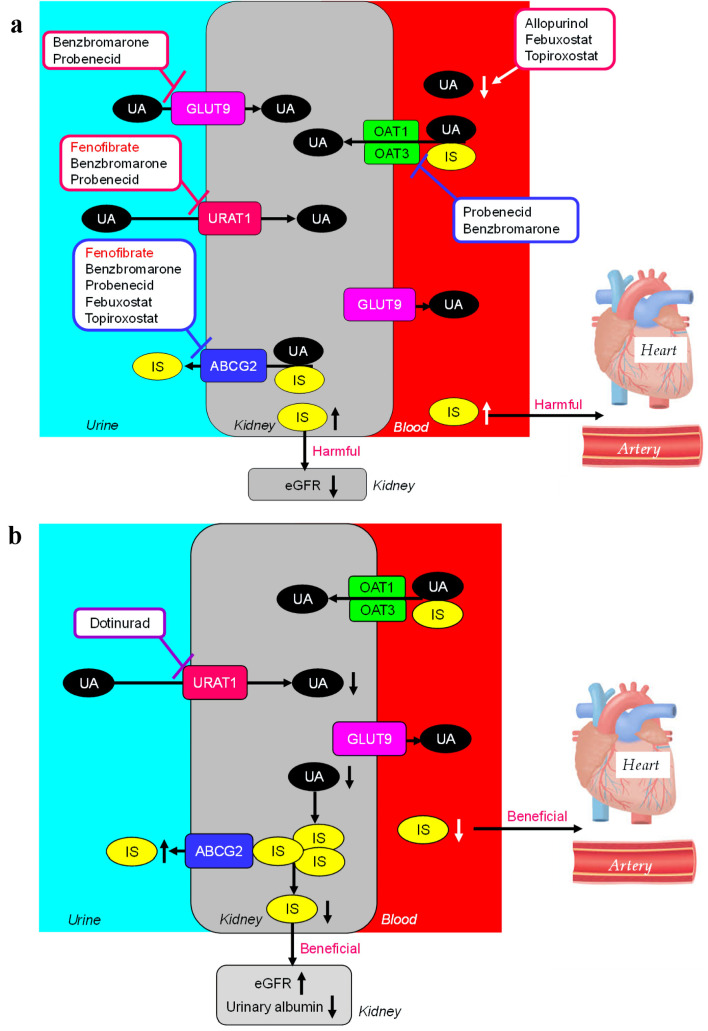
We previously reported that the switching from fenofibrate to the selective peroxisome proliferator-activated receptor (PPAR) α modulator, pemafibrate, increased serum uric acid (UA) levels and reduced estimated glomerular filtration rate (eGFR) in patients with dyslipidemia [1]. Fenofibrate has a property to decrease serum UA by inhibition of urate transporter 1 (URAT1) by its major metabolite [2]. Although fenofibrate was reported to decrease the eGFR [3], the mechanism of fenofibrate-induced renal impairment has been remained unclear. Further, our previous discussion on such issue was premature [1]. Recently, the role of UA transporters has been clarified [4] (Fig. 1a). Renal excretion of UA is the major regulator of serum UA, and renal UA reabsorption is mainly mediated by URAT1 and glucose transporter 9 (GLUT9). Organic anion transporters (OATs) 1, 3 transport UA from the renal interstitial into renal proximal tubule epithelial cells. ATP-binding cassette, subfamily G, 2 (ABCG2) has been identified as a high-capacity UA exporter that mediates renal and/or extrarenal UA excretion. Indoxyl sulfate (IS) is a well-known uremic toxin that accumulates under renal impairment and is involved in the progression of chronic kidney disease (CKD) and cardiovascular disease (CVD), by inducing inflammation and free radical production [5, 6]. IS excretion is also mediated by OAT1/3 and ABCG2 as well as UA excretion [4]. ABCG2 inhibitors, such as febuxostat (xanthin oxidase (XO) inhibitor), caused renal IS accumulation by suppressing its excretion via ABCG2 in rats [7]. Fenofibrate completely inhibits ABCG2 which may lead to increase in renal IS [8], resulting in elevation of eGFR. Another XO inhibitor, topiroxostat, also inhibits ABCG2, however, allopurinol does not inhibit ABCG2. OAT inhibitors such as probenecid (uricosuric drug, URAT1, and GLUT9 inhibitor), suppressed IS uptake into the kidney, leading to increased plasma IS [7]. Increased plasma IS may be harmful to cardiovascular system by inducing inflammation and free radical production. Benzbromarone (uricosuric drug) inhibits OAT1 and OAT3, however, its inhibitory potency for OAT1/3 is lower than those of probenecid [9], which may not lead to an increase in plasma IS. Probenecid and benzbromarone inhibit ABCG2, which may be unfavorably associated with renal function. In short, the inhibition of OAT1/3 and ABCG2 increase IS in plasma and kidney, which may be unfavorably associated with the development of CVD and CKD, respectively. Very recently, we reported that the addition of the selective URAT1 inhibitor dotinurad to highly-evidence-proved drugs to improve CKD such as sodium-glucose cotransporter 2 (SGLT2) inhibitor and a glucagon-like peptide 1 (GLP-1) receptor agonist, improved eGFR in a diabetic patient with CKD stage G4 [10]. Dotinurad inhibits URAT1 specifically, however, does not inhibit ABCG2 [9], and reduces renal UA accumulation, which may increase the transport of renal accumulated IS by ABCG2 because UA may compete with IS for ABCG2 (Fig. 1b). This exquisite crosstalk between URAT1 and ABCG2 induced by dotinurad may be beneficially associated with the development and progression of CKD. Our recent study showed that dotinurad reduced urinary albumin creatinine ratio (UACR) and increased eGFR in patients with CKD [11], supporting our hypothesis. Dotinurad does not inhibit OAT1/3, and then does not increase plasma IS [7]. Possibly, plasma IS may decrease when renal IS decreased because renal excretion is the major regulator of blood UA and IS. This excellent crosstalk between URAT1 and OAT1/3 induced by dotinurad may be favorably associated with the development of CVD. In conclusion, the selective inhibition of URAT1 by dotinurad may induce favorable metabolic changes of uremic toxin, which may be beneficially associated with the development and progression of CKD and CVD.
期刊介绍:
Cardiology Research is an open access, peer-reviewed, international journal. All submissions relating to basic research and clinical practice of cardiology and cardiovascular medicine are in this journal''s scope. This journal focuses on publishing original research and observations in all cardiovascular medicine aspects. Manuscript types include original article, review, case report, short communication, book review, letter to the editor.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
