{"title":"脑脊液分流术治疗Rathke裂隙囊肿经蝶窦引流后难治性迟发性脑积水1例。","authors":"Tetsuo Hashiba, Masahiro Nonaka, Haruka Iwamura, Takamasa Kamei, Junichi Takeda, Akio Asai","doi":"10.1055/s-0043-1768573","DOIUrl":null,"url":null,"abstract":"<p><p>A 75-year-old man presented with bilateral lower limb weakness to our hospital from another clinic. Radiological examinations implied the possibilities of idiopathic normal pressure hydrocephalus (iNPH) and a suprasellar cyst, but both were observed conservatively at that time. Due to the progressive gait disturbance, a lumboperitoneal shunt was implanted 1 year later. The clinical symptoms improved, but the cyst had grown after another year, causing visual impairment. Transsphenoidal drainage of the cyst was performed, but delayed pneumocephalus occurred. Repair surgery was performed with temporary suspension of shunt function, but pneumocephalus relapsed two and a half months after the resumption of shunt flow. In the second repair surgery, the shunt was removed because it was assumed that it would prevent closure of the fistula by lowering intracranial pressure. Two and a half months later, after confirming involution of the cyst and no pneumocephalus, a ventriculoperitoneal shunt was implanted, and cerebrospinal fluid (CSF) leakage has not relapsed since then. The coexistence of idiopathic normal pressure hydrocephalus (iNPH) and Rathke's cleft cyst (RCC) is rare, but it can occur. RCC can be cured by simple drainage, but delayed pneumocephalus can occur in cases whose intracranial pressure decreases due to CSF shunting. When simple drainage without sellar reconstruction for RCC is attempted after CSF shunting for coexistent iNPH, attention should be paid to changes in intracranial pressure, and it is desirable to stop the flow of the shunt for a certain period.</p>","PeriodicalId":8521,"journal":{"name":"Asian Journal of Neurosurgery","volume":"18 2","pages":"342-346"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/46/75/10-1055-s-0043-1768573.PMC10310442.pdf","citationCount":"0","resultStr":"{\"title\":\"Refractory Delayed Pneumocephalus after Transsphenoidal Cyst Drainage for Rathke's Cleft Cyst in a Patient with a Cerebrospinal Fluid Shunt.\",\"authors\":\"Tetsuo Hashiba, Masahiro Nonaka, Haruka Iwamura, Takamasa Kamei, Junichi Takeda, Akio Asai\",\"doi\":\"10.1055/s-0043-1768573\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>A 75-year-old man presented with bilateral lower limb weakness to our hospital from another clinic. Radiological examinations implied the possibilities of idiopathic normal pressure hydrocephalus (iNPH) and a suprasellar cyst, but both were observed conservatively at that time. Due to the progressive gait disturbance, a lumboperitoneal shunt was implanted 1 year later. The clinical symptoms improved, but the cyst had grown after another year, causing visual impairment. Transsphenoidal drainage of the cyst was performed, but delayed pneumocephalus occurred. Repair surgery was performed with temporary suspension of shunt function, but pneumocephalus relapsed two and a half months after the resumption of shunt flow. In the second repair surgery, the shunt was removed because it was assumed that it would prevent closure of the fistula by lowering intracranial pressure. Two and a half months later, after confirming involution of the cyst and no pneumocephalus, a ventriculoperitoneal shunt was implanted, and cerebrospinal fluid (CSF) leakage has not relapsed since then. The coexistence of idiopathic normal pressure hydrocephalus (iNPH) and Rathke's cleft cyst (RCC) is rare, but it can occur. RCC can be cured by simple drainage, but delayed pneumocephalus can occur in cases whose intracranial pressure decreases due to CSF shunting. When simple drainage without sellar reconstruction for RCC is attempted after CSF shunting for coexistent iNPH, attention should be paid to changes in intracranial pressure, and it is desirable to stop the flow of the shunt for a certain period.</p>\",\"PeriodicalId\":8521,\"journal\":{\"name\":\"Asian Journal of Neurosurgery\",\"volume\":\"18 2\",\"pages\":\"342-346\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/46/75/10-1055-s-0043-1768573.PMC10310442.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Asian Journal of Neurosurgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0043-1768573\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asian Journal of Neurosurgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0043-1768573","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Refractory Delayed Pneumocephalus after Transsphenoidal Cyst Drainage for Rathke's Cleft Cyst in a Patient with a Cerebrospinal Fluid Shunt.
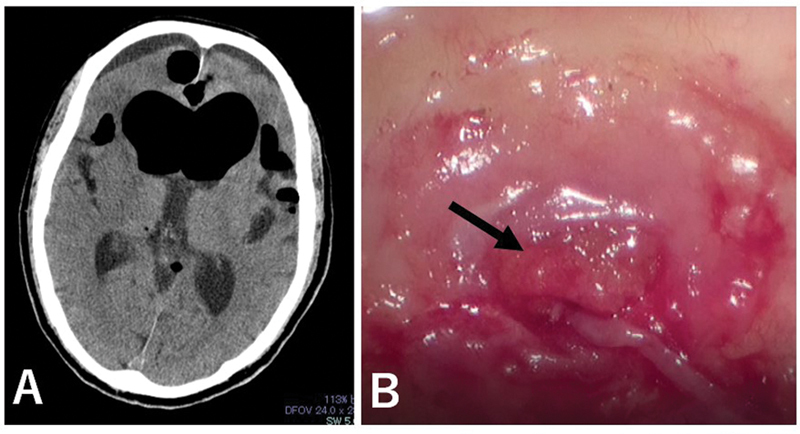
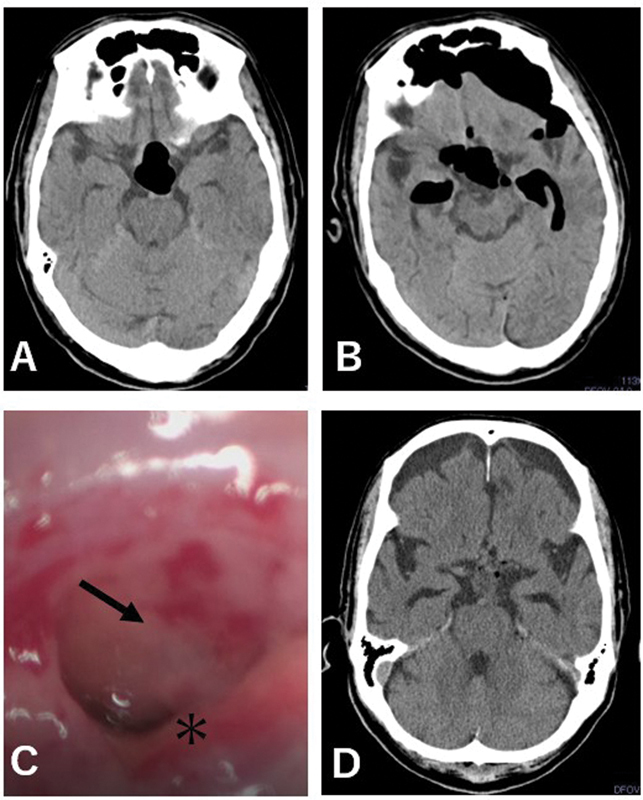
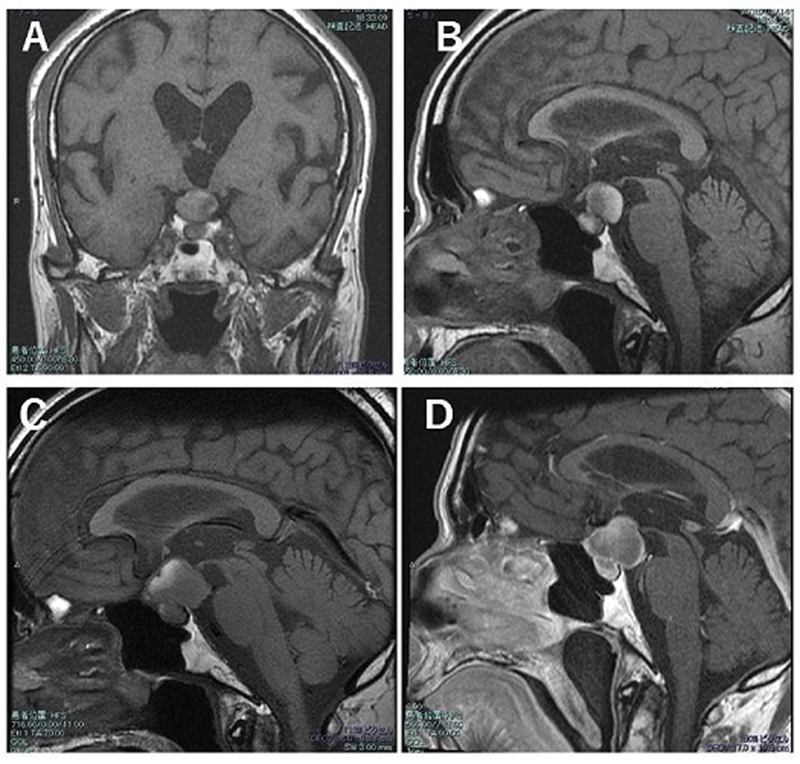
A 75-year-old man presented with bilateral lower limb weakness to our hospital from another clinic. Radiological examinations implied the possibilities of idiopathic normal pressure hydrocephalus (iNPH) and a suprasellar cyst, but both were observed conservatively at that time. Due to the progressive gait disturbance, a lumboperitoneal shunt was implanted 1 year later. The clinical symptoms improved, but the cyst had grown after another year, causing visual impairment. Transsphenoidal drainage of the cyst was performed, but delayed pneumocephalus occurred. Repair surgery was performed with temporary suspension of shunt function, but pneumocephalus relapsed two and a half months after the resumption of shunt flow. In the second repair surgery, the shunt was removed because it was assumed that it would prevent closure of the fistula by lowering intracranial pressure. Two and a half months later, after confirming involution of the cyst and no pneumocephalus, a ventriculoperitoneal shunt was implanted, and cerebrospinal fluid (CSF) leakage has not relapsed since then. The coexistence of idiopathic normal pressure hydrocephalus (iNPH) and Rathke's cleft cyst (RCC) is rare, but it can occur. RCC can be cured by simple drainage, but delayed pneumocephalus can occur in cases whose intracranial pressure decreases due to CSF shunting. When simple drainage without sellar reconstruction for RCC is attempted after CSF shunting for coexistent iNPH, attention should be paid to changes in intracranial pressure, and it is desirable to stop the flow of the shunt for a certain period.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
