Majid Rezvani, Jamalodin Asadi, Arman Sourani, Mina Foroughi, Donya Sheibani Tehrani
{"title":"创伤性脊柱损伤后韧带滑脱过程中骨折内椎弓根螺钉置入:一项随机临床试验。","authors":"Majid Rezvani, Jamalodin Asadi, Arman Sourani, Mina Foroughi, Donya Sheibani Tehrani","doi":"10.13004/kjnt.2023.19.e9","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To investigate the efficacy and safety of two different techniques for spinal ligamentotaxis. Spine ligamentotaxis reduces the number of retropulsed bone fragments in the fractured vertebrae. Two different ligamentotaxis techniques require clinical evaluation.</p><p><strong>Methods: </strong>This was a randomized clinical trial. The case group was defined as one pedicular screw insertion into a fractured vertebra, and the control group as a no-pedicular screw in the index vertebra. Spine biomechanical values were defined as primary outcomes and complications as secondary outcomes.</p><p><strong>Results: </strong>A total of 105 patients were enrolled; 23 were excluded for multiple reasons, and the remaining were randomly allocated into the case (n=40) and control (n=42) groups. The patients were followed up and analyzed (n=56). The postoperative mid-sagittal diameter of the vertebral canal (MSD), kyphotic deformity correction, and restoration of the anterior height of the fractured vertebrae showed equal results in both groups. Postoperative retropulsion percentage and pain were significantly lower in the case group than in the control group (<i>p</i>=0.003 and <i>p</i>=0.004, respectively). There were no group preferences for early or long-term postoperative complications.</p><p><strong>Conclusions: </strong>Regarding clinical and imaging properties, inserting one extra pedicular screw in a fractured vertebra during ligamentotaxis results in better retropulsion reduction and lower postoperative pain.</p>","PeriodicalId":36879,"journal":{"name":"Korean Journal of Neurotrauma","volume":"19 1","pages":"90-102"},"PeriodicalIF":0.0000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c9/82/kjn-19-90.PMC10083448.pdf","citationCount":"4","resultStr":"{\"title\":\"In-Fracture Pedicular Screw Placement During Ligamentotaxis Following Traumatic Spine Injuries, a Randomized Clinical Trial on Outcomes.\",\"authors\":\"Majid Rezvani, Jamalodin Asadi, Arman Sourani, Mina Foroughi, Donya Sheibani Tehrani\",\"doi\":\"10.13004/kjnt.2023.19.e9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To investigate the efficacy and safety of two different techniques for spinal ligamentotaxis. Spine ligamentotaxis reduces the number of retropulsed bone fragments in the fractured vertebrae. Two different ligamentotaxis techniques require clinical evaluation.</p><p><strong>Methods: </strong>This was a randomized clinical trial. The case group was defined as one pedicular screw insertion into a fractured vertebra, and the control group as a no-pedicular screw in the index vertebra. Spine biomechanical values were defined as primary outcomes and complications as secondary outcomes.</p><p><strong>Results: </strong>A total of 105 patients were enrolled; 23 were excluded for multiple reasons, and the remaining were randomly allocated into the case (n=40) and control (n=42) groups. The patients were followed up and analyzed (n=56). The postoperative mid-sagittal diameter of the vertebral canal (MSD), kyphotic deformity correction, and restoration of the anterior height of the fractured vertebrae showed equal results in both groups. Postoperative retropulsion percentage and pain were significantly lower in the case group than in the control group (<i>p</i>=0.003 and <i>p</i>=0.004, respectively). There were no group preferences for early or long-term postoperative complications.</p><p><strong>Conclusions: </strong>Regarding clinical and imaging properties, inserting one extra pedicular screw in a fractured vertebra during ligamentotaxis results in better retropulsion reduction and lower postoperative pain.</p>\",\"PeriodicalId\":36879,\"journal\":{\"name\":\"Korean Journal of Neurotrauma\",\"volume\":\"19 1\",\"pages\":\"90-102\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c9/82/kjn-19-90.PMC10083448.pdf\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Korean Journal of Neurotrauma\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.13004/kjnt.2023.19.e9\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Neurotrauma","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.13004/kjnt.2023.19.e9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
In-Fracture Pedicular Screw Placement During Ligamentotaxis Following Traumatic Spine Injuries, a Randomized Clinical Trial on Outcomes.
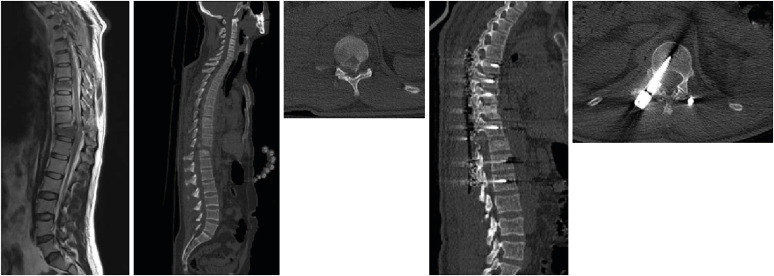
Objective: To investigate the efficacy and safety of two different techniques for spinal ligamentotaxis. Spine ligamentotaxis reduces the number of retropulsed bone fragments in the fractured vertebrae. Two different ligamentotaxis techniques require clinical evaluation.
Methods: This was a randomized clinical trial. The case group was defined as one pedicular screw insertion into a fractured vertebra, and the control group as a no-pedicular screw in the index vertebra. Spine biomechanical values were defined as primary outcomes and complications as secondary outcomes.
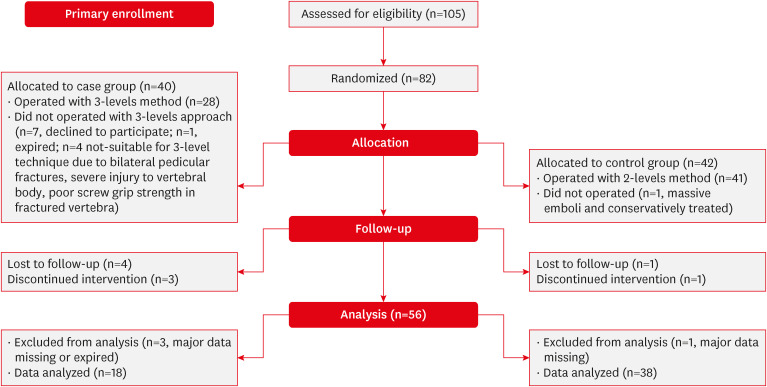
Results: A total of 105 patients were enrolled; 23 were excluded for multiple reasons, and the remaining were randomly allocated into the case (n=40) and control (n=42) groups. The patients were followed up and analyzed (n=56). The postoperative mid-sagittal diameter of the vertebral canal (MSD), kyphotic deformity correction, and restoration of the anterior height of the fractured vertebrae showed equal results in both groups. Postoperative retropulsion percentage and pain were significantly lower in the case group than in the control group (p=0.003 and p=0.004, respectively). There were no group preferences for early or long-term postoperative complications.
Conclusions: Regarding clinical and imaging properties, inserting one extra pedicular screw in a fractured vertebra during ligamentotaxis results in better retropulsion reduction and lower postoperative pain.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
