{"title":"定量血流比例引导下完全血运重建术治疗st段抬高型心肌梗死和多血管疾病的有效性和安全性:一项随机对照试验","authors":"Jing Zhang, Mingyan Yao, Xinwei Jia, Huiping Feng, Jingjing Fu, Wei Tang, Hongliang Cong","doi":"10.5603/CJ.a2021.0111","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In patients with ST-segment elevation myocardial infarction (STEMI) and multivessel disease (MVD), the treatment strategy for non-infarct-related artery (non-IRA) remains controversial. Quantitative flow ratio (QFR) is a new angiography-based physiological assessment index. However, there is little evidence on the practical clinical application of QFR.</p><p><strong>Methods: </strong>Two hundred and twenty-nine patients with STEMI and MVD were recruited for this study. Patients were randomly assigned to either receive QFR-guided complete revascularization (QFR-G-CR) of non-IRA or receive no further invasive treatment. The primary (1°) endpoint analyzed included death due to all causes, non-fatal myocardial infarction (MI), and ischemia-induced revascularization at 12 months post-surgery. Secondary (2°) endpoints included cardiovascular death, unstable angina, stent thrombosis, New York Heart Association (NYHA) class IV heart failure, and stroke at 1 year post surgery. Massive bleeding and contrast-associated acute kidney injury (CAKI) were used as safety endpoints.</p><p><strong>Results: </strong>Around the 12 month follow up, the 1o outcome was recorded in 11/115 patients (9.6%) in the QFR-G-CR population, relative to 23/114 patients (20.1%) in the IRA-only PCI population (hazard ratio [HR]: 0.45; 95% confidence interval [CI]: 0.22-0.92; p = 0.025). Unstable angina in 6 (5.2%) and 16 (14.0%) patients (HR: 0.36; 95% CI: 0.14-0.92; p = 0.026), respectively. No marked alterations were found in the massive bleeding and CAKI categories.</p><p><strong>Conclusions: </strong>In conclusion, STEMI and MVD patients can benefit from QFR-G-CR of non-IRA lesions in the initial stages of acute MI. This can help reduce incidences of major adverse cardiovascular events and unstable angina, relative to IRA treatment only. Chinese Clinical Trial Registration number: ChiCTR2100044120.</p>","PeriodicalId":9492,"journal":{"name":"Cardiology journal","volume":"30 2","pages":"178-187"},"PeriodicalIF":1.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e8/3d/cardj-30-2-178.PMC10129263.pdf","citationCount":"4","resultStr":"{\"title\":\"The efficacy and safety of quantitative flow ratio-guided complete revascularization in patients with ST-segment elevation myocardial infarction and multivessel disease: A pilot randomized controlled trial.\",\"authors\":\"Jing Zhang, Mingyan Yao, Xinwei Jia, Huiping Feng, Jingjing Fu, Wei Tang, Hongliang Cong\",\"doi\":\"10.5603/CJ.a2021.0111\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In patients with ST-segment elevation myocardial infarction (STEMI) and multivessel disease (MVD), the treatment strategy for non-infarct-related artery (non-IRA) remains controversial. Quantitative flow ratio (QFR) is a new angiography-based physiological assessment index. However, there is little evidence on the practical clinical application of QFR.</p><p><strong>Methods: </strong>Two hundred and twenty-nine patients with STEMI and MVD were recruited for this study. Patients were randomly assigned to either receive QFR-guided complete revascularization (QFR-G-CR) of non-IRA or receive no further invasive treatment. The primary (1°) endpoint analyzed included death due to all causes, non-fatal myocardial infarction (MI), and ischemia-induced revascularization at 12 months post-surgery. Secondary (2°) endpoints included cardiovascular death, unstable angina, stent thrombosis, New York Heart Association (NYHA) class IV heart failure, and stroke at 1 year post surgery. Massive bleeding and contrast-associated acute kidney injury (CAKI) were used as safety endpoints.</p><p><strong>Results: </strong>Around the 12 month follow up, the 1o outcome was recorded in 11/115 patients (9.6%) in the QFR-G-CR population, relative to 23/114 patients (20.1%) in the IRA-only PCI population (hazard ratio [HR]: 0.45; 95% confidence interval [CI]: 0.22-0.92; p = 0.025). Unstable angina in 6 (5.2%) and 16 (14.0%) patients (HR: 0.36; 95% CI: 0.14-0.92; p = 0.026), respectively. No marked alterations were found in the massive bleeding and CAKI categories.</p><p><strong>Conclusions: </strong>In conclusion, STEMI and MVD patients can benefit from QFR-G-CR of non-IRA lesions in the initial stages of acute MI. This can help reduce incidences of major adverse cardiovascular events and unstable angina, relative to IRA treatment only. Chinese Clinical Trial Registration number: ChiCTR2100044120.</p>\",\"PeriodicalId\":9492,\"journal\":{\"name\":\"Cardiology journal\",\"volume\":\"30 2\",\"pages\":\"178-187\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e8/3d/cardj-30-2-178.PMC10129263.pdf\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5603/CJ.a2021.0111\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5603/CJ.a2021.0111","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
The efficacy and safety of quantitative flow ratio-guided complete revascularization in patients with ST-segment elevation myocardial infarction and multivessel disease: A pilot randomized controlled trial.
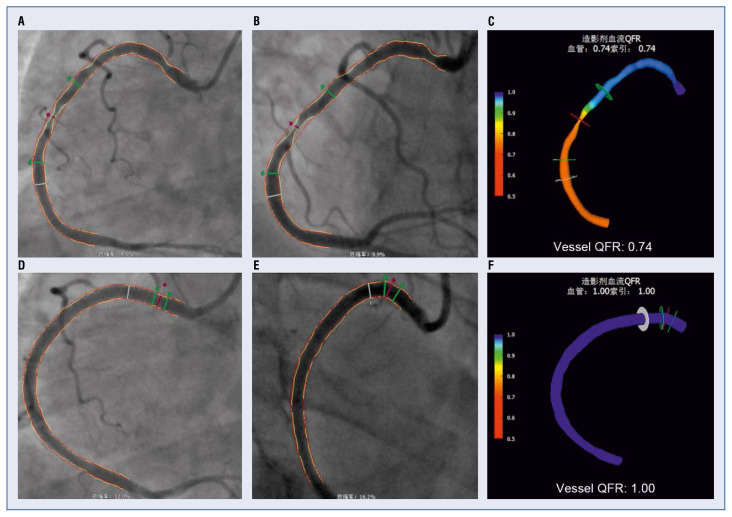
Background: In patients with ST-segment elevation myocardial infarction (STEMI) and multivessel disease (MVD), the treatment strategy for non-infarct-related artery (non-IRA) remains controversial. Quantitative flow ratio (QFR) is a new angiography-based physiological assessment index. However, there is little evidence on the practical clinical application of QFR.
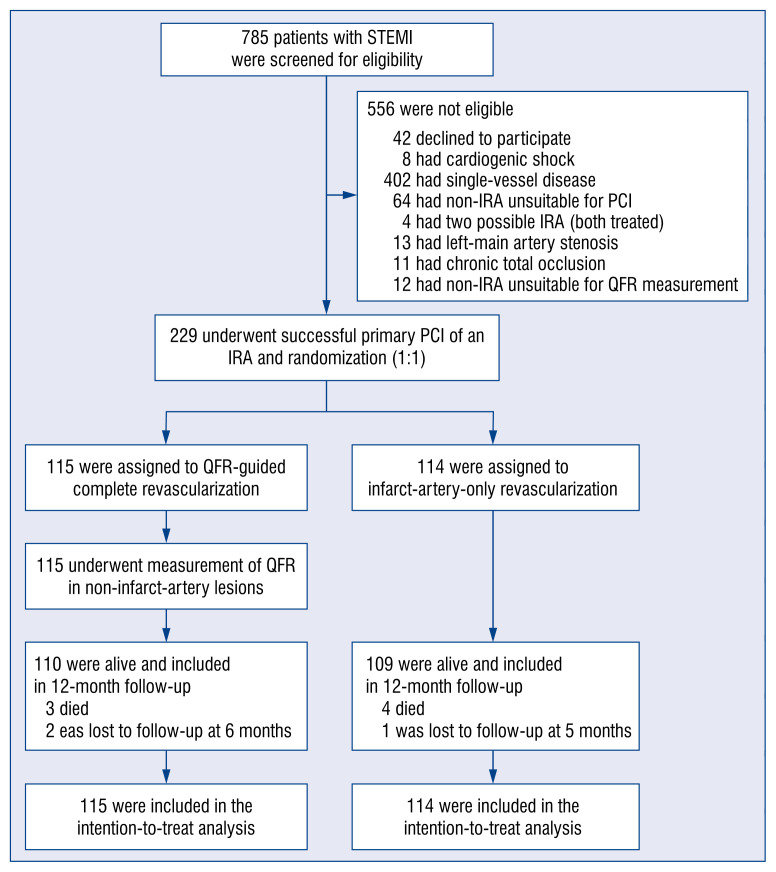
Methods: Two hundred and twenty-nine patients with STEMI and MVD were recruited for this study. Patients were randomly assigned to either receive QFR-guided complete revascularization (QFR-G-CR) of non-IRA or receive no further invasive treatment. The primary (1°) endpoint analyzed included death due to all causes, non-fatal myocardial infarction (MI), and ischemia-induced revascularization at 12 months post-surgery. Secondary (2°) endpoints included cardiovascular death, unstable angina, stent thrombosis, New York Heart Association (NYHA) class IV heart failure, and stroke at 1 year post surgery. Massive bleeding and contrast-associated acute kidney injury (CAKI) were used as safety endpoints.
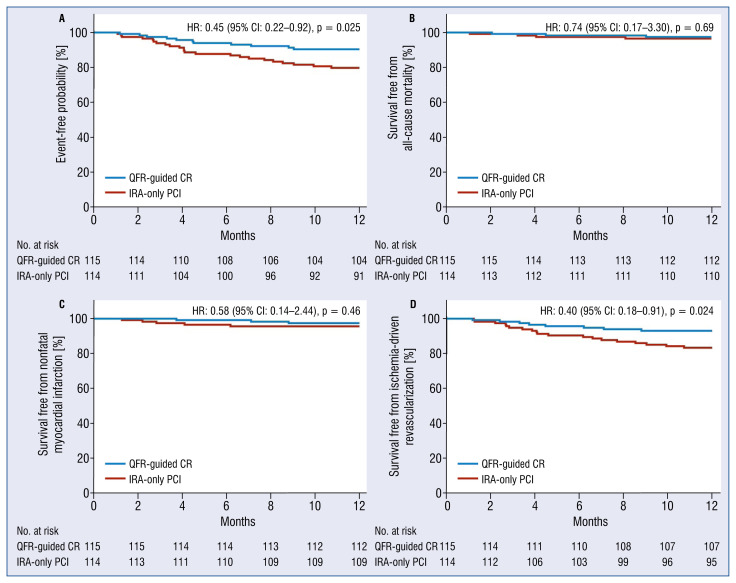
Results: Around the 12 month follow up, the 1o outcome was recorded in 11/115 patients (9.6%) in the QFR-G-CR population, relative to 23/114 patients (20.1%) in the IRA-only PCI population (hazard ratio [HR]: 0.45; 95% confidence interval [CI]: 0.22-0.92; p = 0.025). Unstable angina in 6 (5.2%) and 16 (14.0%) patients (HR: 0.36; 95% CI: 0.14-0.92; p = 0.026), respectively. No marked alterations were found in the massive bleeding and CAKI categories.
Conclusions: In conclusion, STEMI and MVD patients can benefit from QFR-G-CR of non-IRA lesions in the initial stages of acute MI. This can help reduce incidences of major adverse cardiovascular events and unstable angina, relative to IRA treatment only. Chinese Clinical Trial Registration number: ChiCTR2100044120.
期刊介绍:
Cardiology Journal is a scientific, peer-reviewed journal covering a broad spectrum of topics in cardiology. The journal has been published since 1994 and over the years it has become an internationally recognized journal of cardiological and medical community.
Cardiology Journal is the journal for practicing cardiologists, researchers, and young trainees benefiting from broad spectrum of useful educational content.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
