{"title":"在颅内压监测下行血肿引流加硬膜外补血治疗慢性硬膜下血肿自发性低血压2例。","authors":"Toshitsugu Terakado, Akibumi Omi, Yuji Matsumaru, Eiichi Ishikawa","doi":"10.2176/jns-nmc.2022-0356","DOIUrl":null,"url":null,"abstract":"<p><p>Both chronic subdural hematoma (CSDH) and spontaneous intracranial hypotension (SIH) cause headaches. However, the etiologies are different: SIH headache is caused by decreased intracranial pressure (ICP), whereas CSDH headache results from increased ICP. Moreover, CSDH is treated by hematoma drainage, while SIH is treated by epidural blood patch (EBP). Treatment for the cases of combined SIH and CSDH is not well-established. Herein, we report two cases wherein ICP was monitored and safely controlled by EBP after hematoma drainage. Case 1: A 55-year-old man with progressive consciousness disturbance was diagnosed with bilateral CSDH. He underwent bilateral hematoma drainage; however, the headache became apparent during standing. We diagnosed SIH by diffuse pachymeningeal enhancement on brain MRI and epidural contrast medium leakage on CT myelography. Due to the re-enlargement of bilateral CSDH, we performed EBP after hematoma drainage and ICP monitor insertion. Finally, the headache and bilateral CSDH were resolved. Case 2: A 54-year-old man with persistent headache was diagnosed with bilateral CSDH. He underwent multiple hematoma drainage sessions. However, headache on standing persisted. We diagnosed SIH by diffuse pachymeningeal enhancement on brain MRI and epidural contrast medium leakage on CT myelography. Due to the re-enlargement of the left CSDH, we performed EBP after left hematoma drainage and ICP monitor insertion. Finally, the headache and bilateral CSDH were resolved. EBP after hematoma drainage and ICP monitoring was useful for SIH with bilateral CSDH. By monitoring ICP before EBP, the ICP was safely controlled and CSDH was resolved.</p>","PeriodicalId":19260,"journal":{"name":"NMC Case Report Journal","volume":"10 ","pages":"93-98"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d9/ef/2188-4226-10-0093.PMC10149143.pdf","citationCount":"0","resultStr":"{\"title\":\"Two Cases of Chronic Subdural Hematoma with Spontaneous Intracranial Hypotention Treated with Hematoma Drainage Followed by Epidural Blood Patch Under Intracranial Pressure Monitoring.\",\"authors\":\"Toshitsugu Terakado, Akibumi Omi, Yuji Matsumaru, Eiichi Ishikawa\",\"doi\":\"10.2176/jns-nmc.2022-0356\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Both chronic subdural hematoma (CSDH) and spontaneous intracranial hypotension (SIH) cause headaches. However, the etiologies are different: SIH headache is caused by decreased intracranial pressure (ICP), whereas CSDH headache results from increased ICP. Moreover, CSDH is treated by hematoma drainage, while SIH is treated by epidural blood patch (EBP). Treatment for the cases of combined SIH and CSDH is not well-established. Herein, we report two cases wherein ICP was monitored and safely controlled by EBP after hematoma drainage. Case 1: A 55-year-old man with progressive consciousness disturbance was diagnosed with bilateral CSDH. He underwent bilateral hematoma drainage; however, the headache became apparent during standing. We diagnosed SIH by diffuse pachymeningeal enhancement on brain MRI and epidural contrast medium leakage on CT myelography. Due to the re-enlargement of bilateral CSDH, we performed EBP after hematoma drainage and ICP monitor insertion. Finally, the headache and bilateral CSDH were resolved. Case 2: A 54-year-old man with persistent headache was diagnosed with bilateral CSDH. He underwent multiple hematoma drainage sessions. However, headache on standing persisted. We diagnosed SIH by diffuse pachymeningeal enhancement on brain MRI and epidural contrast medium leakage on CT myelography. Due to the re-enlargement of the left CSDH, we performed EBP after left hematoma drainage and ICP monitor insertion. Finally, the headache and bilateral CSDH were resolved. EBP after hematoma drainage and ICP monitoring was useful for SIH with bilateral CSDH. By monitoring ICP before EBP, the ICP was safely controlled and CSDH was resolved.</p>\",\"PeriodicalId\":19260,\"journal\":{\"name\":\"NMC Case Report Journal\",\"volume\":\"10 \",\"pages\":\"93-98\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d9/ef/2188-4226-10-0093.PMC10149143.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NMC Case Report Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2176/jns-nmc.2022-0356\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NMC Case Report Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2022-0356","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Two Cases of Chronic Subdural Hematoma with Spontaneous Intracranial Hypotention Treated with Hematoma Drainage Followed by Epidural Blood Patch Under Intracranial Pressure Monitoring.
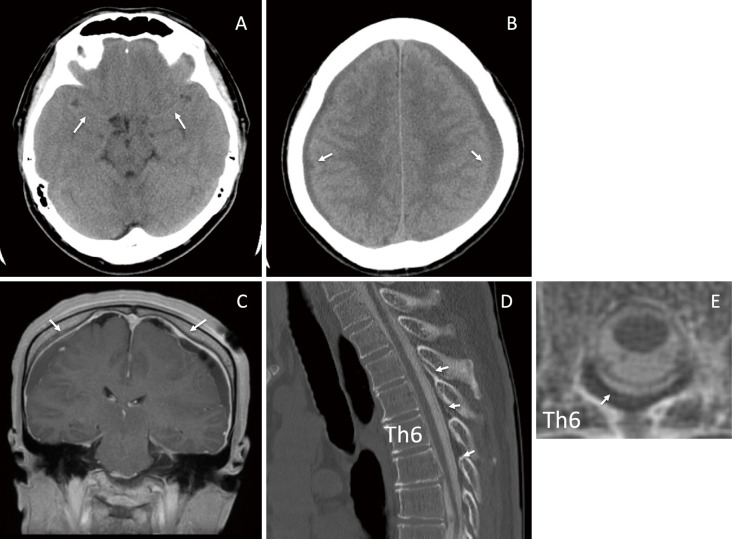
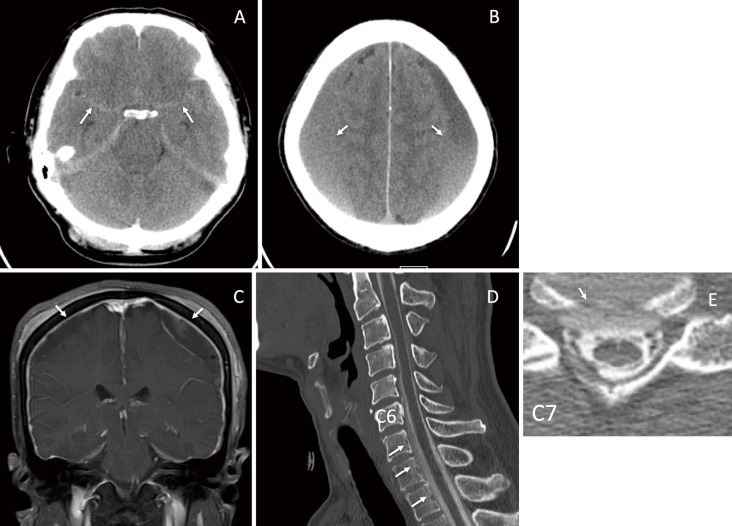
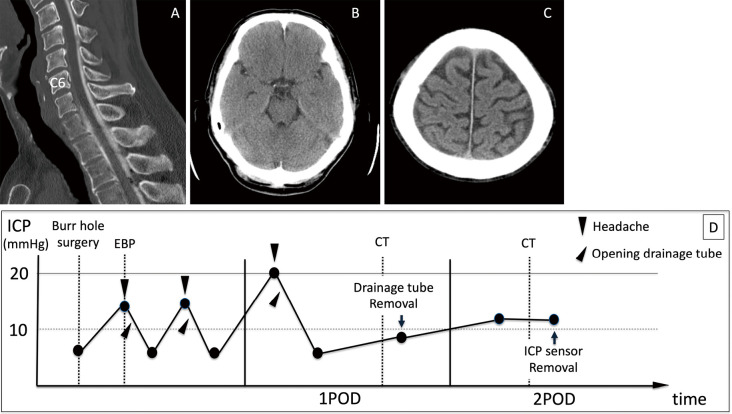
Both chronic subdural hematoma (CSDH) and spontaneous intracranial hypotension (SIH) cause headaches. However, the etiologies are different: SIH headache is caused by decreased intracranial pressure (ICP), whereas CSDH headache results from increased ICP. Moreover, CSDH is treated by hematoma drainage, while SIH is treated by epidural blood patch (EBP). Treatment for the cases of combined SIH and CSDH is not well-established. Herein, we report two cases wherein ICP was monitored and safely controlled by EBP after hematoma drainage. Case 1: A 55-year-old man with progressive consciousness disturbance was diagnosed with bilateral CSDH. He underwent bilateral hematoma drainage; however, the headache became apparent during standing. We diagnosed SIH by diffuse pachymeningeal enhancement on brain MRI and epidural contrast medium leakage on CT myelography. Due to the re-enlargement of bilateral CSDH, we performed EBP after hematoma drainage and ICP monitor insertion. Finally, the headache and bilateral CSDH were resolved. Case 2: A 54-year-old man with persistent headache was diagnosed with bilateral CSDH. He underwent multiple hematoma drainage sessions. However, headache on standing persisted. We diagnosed SIH by diffuse pachymeningeal enhancement on brain MRI and epidural contrast medium leakage on CT myelography. Due to the re-enlargement of the left CSDH, we performed EBP after left hematoma drainage and ICP monitor insertion. Finally, the headache and bilateral CSDH were resolved. EBP after hematoma drainage and ICP monitoring was useful for SIH with bilateral CSDH. By monitoring ICP before EBP, the ICP was safely controlled and CSDH was resolved.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
