Andrew K Chang, Jakrin Kewcharoen, Danielle M Henkel, Purvi Parwani, Dmitry Abramov
{"title":"心肌收缩率不能预测急性收缩性心力衰竭的临床结果:一份简短报告。","authors":"Andrew K Chang, Jakrin Kewcharoen, Danielle M Henkel, Purvi Parwani, Dmitry Abramov","doi":"10.4103/jcecho.jcecho_53_22","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The utility of myocardial contraction fraction (MCF), a volumetric measure of myocardial shortening, has not been well evaluated in patients with systolic heart failure (SHF).</p><p><strong>Materials and methods: </strong>A single-center, retrospective cohort study of all adults admitted with acute SHF from 2013 to 2018 at an academic medical center. A chart review was performed to identify key echocardiographic transthoracic echocardiogram (TTE), laboratory, and demographic characteristics. MCF was calculated based on M-mode measurements of estimated stroke volume and myocardial volume based on admission TTE. The primary outcome was 30-day combined all-cause readmission/mortality and 365-day all-cause mortality.</p><p><strong>Results: </strong>A total of 1282 patients were analyzed. The 30-day composite outcome occurred in 310 patients (24.2%), and all-cause death at 365 days occurred in 375 patients (29.3%). There was a weak correlation between the visually estimated ejection fraction (EF) and MCF (<i>r</i> = 0.356, <i>P</i> < 0.001). Neither MCF nor EF was associated with either component of the primary outcome. Other parameters on TTE that were associated with higher risk of primary outcome were higher tricuspid regurgitation (TR) velocity, larger left atrial (LA) diameter, and moderate or greater TR and mitral regurgitation (MR).</p><p><strong>Conclusion: </strong>Echocardiographic predictors of postdischarge adverse events among patients hospitalized with acute SHF include higher TR velocity, larger LA diameter, and at least moderate MR or TR. MCF does not correlate well with visually assessed EF among patients with acute SHF, and neither MCF nor EF provides prognostic information in this population.</p>","PeriodicalId":15191,"journal":{"name":"Journal of Cardiovascular Echography","volume":"33 1","pages":"27-29"},"PeriodicalIF":1.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10328125/pdf/","citationCount":"0","resultStr":"{\"title\":\"Myocardial Contraction Fraction is not a Predictor of Clinical Outcomes in Acute Systolic Heart Failure: A Brief Report.\",\"authors\":\"Andrew K Chang, Jakrin Kewcharoen, Danielle M Henkel, Purvi Parwani, Dmitry Abramov\",\"doi\":\"10.4103/jcecho.jcecho_53_22\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The utility of myocardial contraction fraction (MCF), a volumetric measure of myocardial shortening, has not been well evaluated in patients with systolic heart failure (SHF).</p><p><strong>Materials and methods: </strong>A single-center, retrospective cohort study of all adults admitted with acute SHF from 2013 to 2018 at an academic medical center. A chart review was performed to identify key echocardiographic transthoracic echocardiogram (TTE), laboratory, and demographic characteristics. MCF was calculated based on M-mode measurements of estimated stroke volume and myocardial volume based on admission TTE. The primary outcome was 30-day combined all-cause readmission/mortality and 365-day all-cause mortality.</p><p><strong>Results: </strong>A total of 1282 patients were analyzed. The 30-day composite outcome occurred in 310 patients (24.2%), and all-cause death at 365 days occurred in 375 patients (29.3%). There was a weak correlation between the visually estimated ejection fraction (EF) and MCF (<i>r</i> = 0.356, <i>P</i> < 0.001). Neither MCF nor EF was associated with either component of the primary outcome. Other parameters on TTE that were associated with higher risk of primary outcome were higher tricuspid regurgitation (TR) velocity, larger left atrial (LA) diameter, and moderate or greater TR and mitral regurgitation (MR).</p><p><strong>Conclusion: </strong>Echocardiographic predictors of postdischarge adverse events among patients hospitalized with acute SHF include higher TR velocity, larger LA diameter, and at least moderate MR or TR. MCF does not correlate well with visually assessed EF among patients with acute SHF, and neither MCF nor EF provides prognostic information in this population.</p>\",\"PeriodicalId\":15191,\"journal\":{\"name\":\"Journal of Cardiovascular Echography\",\"volume\":\"33 1\",\"pages\":\"27-29\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10328125/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiovascular Echography\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/jcecho.jcecho_53_22\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/5/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Echography","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcecho.jcecho_53_22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/5/29 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Myocardial Contraction Fraction is not a Predictor of Clinical Outcomes in Acute Systolic Heart Failure: A Brief Report.
Introduction: The utility of myocardial contraction fraction (MCF), a volumetric measure of myocardial shortening, has not been well evaluated in patients with systolic heart failure (SHF).
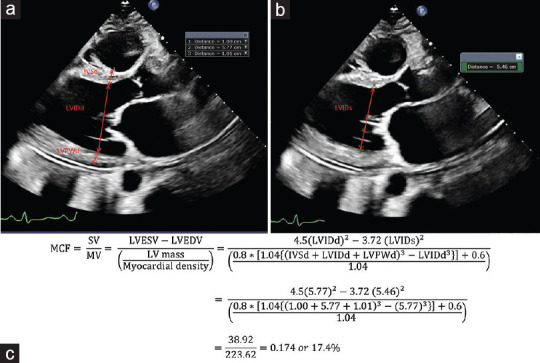
Materials and methods: A single-center, retrospective cohort study of all adults admitted with acute SHF from 2013 to 2018 at an academic medical center. A chart review was performed to identify key echocardiographic transthoracic echocardiogram (TTE), laboratory, and demographic characteristics. MCF was calculated based on M-mode measurements of estimated stroke volume and myocardial volume based on admission TTE. The primary outcome was 30-day combined all-cause readmission/mortality and 365-day all-cause mortality.
Results: A total of 1282 patients were analyzed. The 30-day composite outcome occurred in 310 patients (24.2%), and all-cause death at 365 days occurred in 375 patients (29.3%). There was a weak correlation between the visually estimated ejection fraction (EF) and MCF (r = 0.356, P < 0.001). Neither MCF nor EF was associated with either component of the primary outcome. Other parameters on TTE that were associated with higher risk of primary outcome were higher tricuspid regurgitation (TR) velocity, larger left atrial (LA) diameter, and moderate or greater TR and mitral regurgitation (MR).
Conclusion: Echocardiographic predictors of postdischarge adverse events among patients hospitalized with acute SHF include higher TR velocity, larger LA diameter, and at least moderate MR or TR. MCF does not correlate well with visually assessed EF among patients with acute SHF, and neither MCF nor EF provides prognostic information in this population.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
