Katherine E Mallett, Michael J Taunton, Matthew P Abdel, Rafael J Sierra
{"title":"脱位和解离的双移动部件很容易被遗漏,超过一半的部件无法闭合复位:帮助管理的六个技巧。","authors":"Katherine E Mallett, Michael J Taunton, Matthew P Abdel, Rafael J Sierra","doi":"10.2106/JBJS.OA.22.00108","DOIUrl":null,"url":null,"abstract":"<p><p>Dual-mobility (DM) implants reduce the risk of dislocation in patients who have undergone total hip arthroplasty (THA); however, DM implants are at risk for large-head dislocation and intraprosthetic dissociation (IPD), where the inner femoral head dissociates from the outer polyethylene head. This study aimed to report the incidence of DM dislocation and IPD, evaluate the rate of recognition of IPD before and after reduction, investigate the outcomes of these complications, and provide treatment recommendations for their management.</p><p><strong>Methods: </strong>Between 2010 and 2021, 695 primary and 758 revision THAs were performed with DM constructs at a single institution. There were 44 large-head dislocations (3.0%) and 10 IPDs (0.7%). Four additional IPDs occurred during attempted closed reduction, increasing the IPD incidence to 0.96%. We reviewed prior instability history, dislocation management, success of reduction, recognition of IPD, and subsequent rates of revision and complications. The mean follow-up was 2.5 years.</p><p><strong>Results: </strong>Nine of 10 IPDs were missed at presentation and thus not treated as such. Sixty-three percent of attempted closed reductions in the emergency department failed and led to 4 IPDs and 1 periprosthetic fracture. Reduction success was associated with the following factors: use of general anesthesia with paralysis (p = 0.02), having the reduction performed by an orthopaedist (p = 0.03), and undergoing only 1 reduction attempt (p = 0.015). Two-thirds of dislocations required revision. The rate of redislocation was 33%, and 5 hips required subsequent revision at a mean of 1.8 years after the initial dislocation.</p><p><strong>Conclusions: </strong>We present an evaluation of DM-implant dislocation and dissociation along with management recommendations based on these data. Given the low success and high complication rates of attempted closed reduction and the need for eventual revision, we recommend that all patients with dislocated DM implants be brought to the operating room for closed reduction as well as potential revision if the reduction fails.</p><p><strong>Level of evidence: </strong>Therapeutic Level IV. See Instructions for Authors for a complete description of levels of evidence.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"8 3","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2023-07-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a7/de/jbjsoa-8-e22.00108.PMC10348735.pdf","citationCount":"0","resultStr":"{\"title\":\"Dislocated and Dissociated Dual-Mobility Components Are Easily Missed and More Than Half Fail Closed Reduction: Six Tips to Aid Management.\",\"authors\":\"Katherine E Mallett, Michael J Taunton, Matthew P Abdel, Rafael J Sierra\",\"doi\":\"10.2106/JBJS.OA.22.00108\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Dual-mobility (DM) implants reduce the risk of dislocation in patients who have undergone total hip arthroplasty (THA); however, DM implants are at risk for large-head dislocation and intraprosthetic dissociation (IPD), where the inner femoral head dissociates from the outer polyethylene head. This study aimed to report the incidence of DM dislocation and IPD, evaluate the rate of recognition of IPD before and after reduction, investigate the outcomes of these complications, and provide treatment recommendations for their management.</p><p><strong>Methods: </strong>Between 2010 and 2021, 695 primary and 758 revision THAs were performed with DM constructs at a single institution. There were 44 large-head dislocations (3.0%) and 10 IPDs (0.7%). Four additional IPDs occurred during attempted closed reduction, increasing the IPD incidence to 0.96%. We reviewed prior instability history, dislocation management, success of reduction, recognition of IPD, and subsequent rates of revision and complications. The mean follow-up was 2.5 years.</p><p><strong>Results: </strong>Nine of 10 IPDs were missed at presentation and thus not treated as such. Sixty-three percent of attempted closed reductions in the emergency department failed and led to 4 IPDs and 1 periprosthetic fracture. Reduction success was associated with the following factors: use of general anesthesia with paralysis (p = 0.02), having the reduction performed by an orthopaedist (p = 0.03), and undergoing only 1 reduction attempt (p = 0.015). Two-thirds of dislocations required revision. The rate of redislocation was 33%, and 5 hips required subsequent revision at a mean of 1.8 years after the initial dislocation.</p><p><strong>Conclusions: </strong>We present an evaluation of DM-implant dislocation and dissociation along with management recommendations based on these data. Given the low success and high complication rates of attempted closed reduction and the need for eventual revision, we recommend that all patients with dislocated DM implants be brought to the operating room for closed reduction as well as potential revision if the reduction fails.</p><p><strong>Level of evidence: </strong>Therapeutic Level IV. See Instructions for Authors for a complete description of levels of evidence.</p>\",\"PeriodicalId\":36492,\"journal\":{\"name\":\"JBJS Open Access\",\"volume\":\"8 3\",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2023-07-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a7/de/jbjsoa-8-e22.00108.PMC10348735.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JBJS Open Access\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2106/JBJS.OA.22.00108\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.22.00108","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Dislocated and Dissociated Dual-Mobility Components Are Easily Missed and More Than Half Fail Closed Reduction: Six Tips to Aid Management.
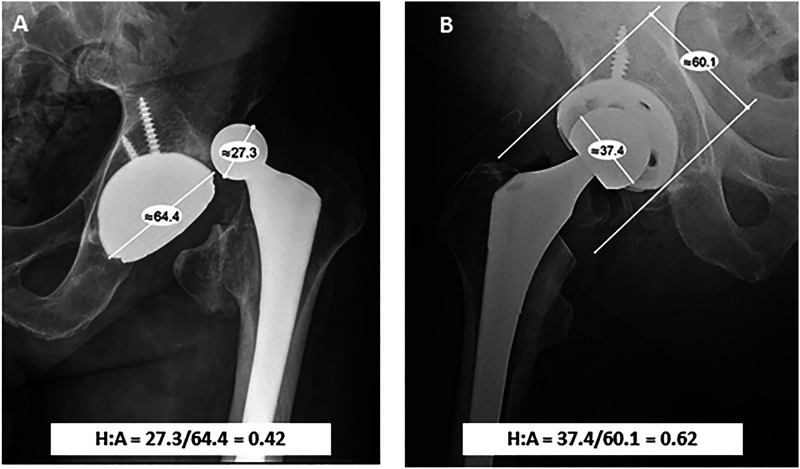
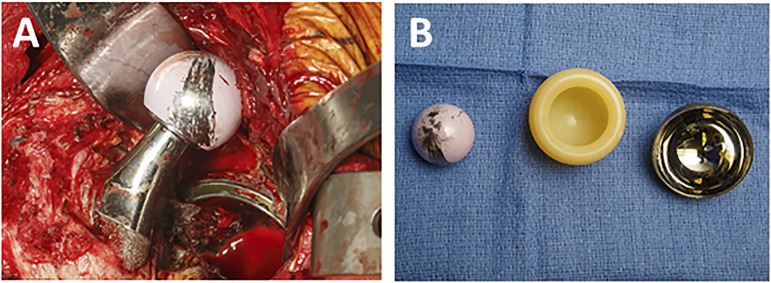
Dual-mobility (DM) implants reduce the risk of dislocation in patients who have undergone total hip arthroplasty (THA); however, DM implants are at risk for large-head dislocation and intraprosthetic dissociation (IPD), where the inner femoral head dissociates from the outer polyethylene head. This study aimed to report the incidence of DM dislocation and IPD, evaluate the rate of recognition of IPD before and after reduction, investigate the outcomes of these complications, and provide treatment recommendations for their management.
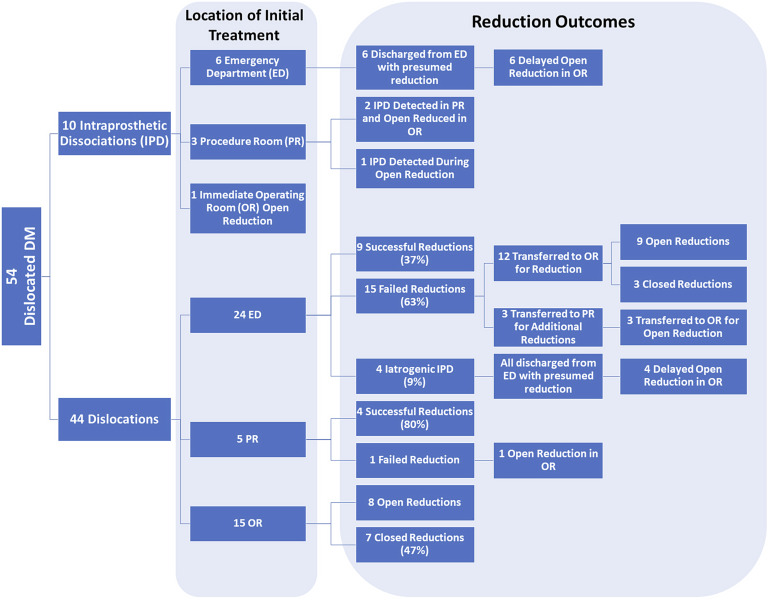
Methods: Between 2010 and 2021, 695 primary and 758 revision THAs were performed with DM constructs at a single institution. There were 44 large-head dislocations (3.0%) and 10 IPDs (0.7%). Four additional IPDs occurred during attempted closed reduction, increasing the IPD incidence to 0.96%. We reviewed prior instability history, dislocation management, success of reduction, recognition of IPD, and subsequent rates of revision and complications. The mean follow-up was 2.5 years.
Results: Nine of 10 IPDs were missed at presentation and thus not treated as such. Sixty-three percent of attempted closed reductions in the emergency department failed and led to 4 IPDs and 1 periprosthetic fracture. Reduction success was associated with the following factors: use of general anesthesia with paralysis (p = 0.02), having the reduction performed by an orthopaedist (p = 0.03), and undergoing only 1 reduction attempt (p = 0.015). Two-thirds of dislocations required revision. The rate of redislocation was 33%, and 5 hips required subsequent revision at a mean of 1.8 years after the initial dislocation.
Conclusions: We present an evaluation of DM-implant dislocation and dissociation along with management recommendations based on these data. Given the low success and high complication rates of attempted closed reduction and the need for eventual revision, we recommend that all patients with dislocated DM implants be brought to the operating room for closed reduction as well as potential revision if the reduction fails.
Level of evidence: Therapeutic Level IV. See Instructions for Authors for a complete description of levels of evidence.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
