Tomoya Yokoyama, Shigeki Sunaga, Hiroyuki Onuki, Kunitoshi Otsuka, Hiroyuki Jimbo
{"title":"颈动脉内膜切除术后与脑高灌注综合征相关的非惊厥性癫痫持续状态1例报告。","authors":"Tomoya Yokoyama, Shigeki Sunaga, Hiroyuki Onuki, Kunitoshi Otsuka, Hiroyuki Jimbo","doi":"10.2176/jns-nmc.2022-0333","DOIUrl":null,"url":null,"abstract":"<p><p>We report a case of a 73-year-old man who developed nonconvulsive status epilepticus as a complication of cerebral hyperperfusion syndrome after carotid endarterectomy for carotid artery stenosis. On postoperative day 1, the patient experienced headaches and vomiting. Resting <i>N</i>-isopropyl-<i>p</i>-[<sup>123</sup>I] iodoamphetamine single-photon emission computed tomography showed increased cerebral blood flow to the entire right hemisphere, and the patient was diagnosed with cerebral hyperperfusion syndrome. He was treated with antihypertensive and antiseizure medications, sedated using propofol, intubated, and placed under mechanical ventilation. On postoperative day 3, computed tomography perfusion imaging showed a reduction in hyperperfusion, and propofol sedation was terminated on postoperative day 4. However, the patient exhibited prolonged impaired awareness and roving eye movements, and long-term video electroencephalographic monitoring revealed electrographic seizures. The patient was diagnosed with nonconvulsive status epilepticus. Propofol sedation was resumed, and the antiseizure medication dose was increased. Subsequently, the state of hyperperfusion in the right hemisphere diminished, and electroencephalographic findings improved, allowing sedation to be terminated on postoperative day 7. The findings from this case suggest that when clinical subtle symptoms, such as impaired awareness and roving eye movements, are observed during treatment of cerebral hyperperfusion syndrome, video electroencephalography should be performed to detect electrographic seizures.</p>","PeriodicalId":19260,"journal":{"name":"NMC Case Report Journal","volume":"10 ","pages":"197-202"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/16/13/2188-4226-10-0197.PMC10351957.pdf","citationCount":"0","resultStr":"{\"title\":\"Nonconvulsive Status Epilepticus Associated with Cerebral Hyperperfusion Syndrome after Carotid Endarterectomy: A Case Report.\",\"authors\":\"Tomoya Yokoyama, Shigeki Sunaga, Hiroyuki Onuki, Kunitoshi Otsuka, Hiroyuki Jimbo\",\"doi\":\"10.2176/jns-nmc.2022-0333\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>We report a case of a 73-year-old man who developed nonconvulsive status epilepticus as a complication of cerebral hyperperfusion syndrome after carotid endarterectomy for carotid artery stenosis. On postoperative day 1, the patient experienced headaches and vomiting. Resting <i>N</i>-isopropyl-<i>p</i>-[<sup>123</sup>I] iodoamphetamine single-photon emission computed tomography showed increased cerebral blood flow to the entire right hemisphere, and the patient was diagnosed with cerebral hyperperfusion syndrome. He was treated with antihypertensive and antiseizure medications, sedated using propofol, intubated, and placed under mechanical ventilation. On postoperative day 3, computed tomography perfusion imaging showed a reduction in hyperperfusion, and propofol sedation was terminated on postoperative day 4. However, the patient exhibited prolonged impaired awareness and roving eye movements, and long-term video electroencephalographic monitoring revealed electrographic seizures. The patient was diagnosed with nonconvulsive status epilepticus. Propofol sedation was resumed, and the antiseizure medication dose was increased. Subsequently, the state of hyperperfusion in the right hemisphere diminished, and electroencephalographic findings improved, allowing sedation to be terminated on postoperative day 7. The findings from this case suggest that when clinical subtle symptoms, such as impaired awareness and roving eye movements, are observed during treatment of cerebral hyperperfusion syndrome, video electroencephalography should be performed to detect electrographic seizures.</p>\",\"PeriodicalId\":19260,\"journal\":{\"name\":\"NMC Case Report Journal\",\"volume\":\"10 \",\"pages\":\"197-202\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/16/13/2188-4226-10-0197.PMC10351957.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NMC Case Report Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2176/jns-nmc.2022-0333\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NMC Case Report Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2022-0333","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Nonconvulsive Status Epilepticus Associated with Cerebral Hyperperfusion Syndrome after Carotid Endarterectomy: A Case Report.
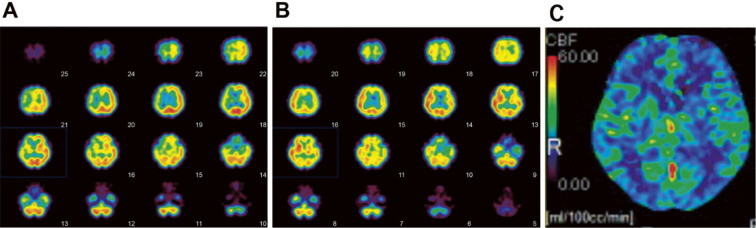
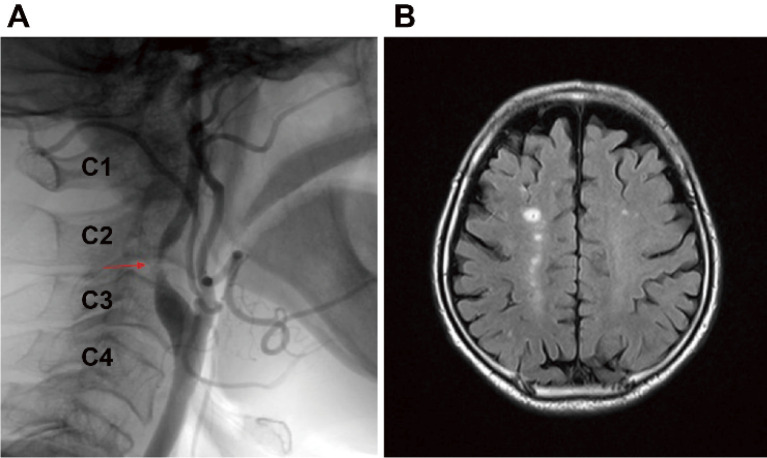
We report a case of a 73-year-old man who developed nonconvulsive status epilepticus as a complication of cerebral hyperperfusion syndrome after carotid endarterectomy for carotid artery stenosis. On postoperative day 1, the patient experienced headaches and vomiting. Resting N-isopropyl-p-[123I] iodoamphetamine single-photon emission computed tomography showed increased cerebral blood flow to the entire right hemisphere, and the patient was diagnosed with cerebral hyperperfusion syndrome. He was treated with antihypertensive and antiseizure medications, sedated using propofol, intubated, and placed under mechanical ventilation. On postoperative day 3, computed tomography perfusion imaging showed a reduction in hyperperfusion, and propofol sedation was terminated on postoperative day 4. However, the patient exhibited prolonged impaired awareness and roving eye movements, and long-term video electroencephalographic monitoring revealed electrographic seizures. The patient was diagnosed with nonconvulsive status epilepticus. Propofol sedation was resumed, and the antiseizure medication dose was increased. Subsequently, the state of hyperperfusion in the right hemisphere diminished, and electroencephalographic findings improved, allowing sedation to be terminated on postoperative day 7. The findings from this case suggest that when clinical subtle symptoms, such as impaired awareness and roving eye movements, are observed during treatment of cerebral hyperperfusion syndrome, video electroencephalography should be performed to detect electrographic seizures.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
