Kento Takahara, Tomoru Miwa, Takashi Iwama, Masahiro Toda
{"title":"经枕幕入路治疗小脑上病变。","authors":"Kento Takahara, Tomoru Miwa, Takashi Iwama, Masahiro Toda","doi":"10.2176/jns-nmc.2022-0363","DOIUrl":null,"url":null,"abstract":"<p><p>The occipital transtentorial approach (OTA), which is often applied for superior cerebellar lesions, has an inevitable risk of homonymous hemianopsia due to the retraction of the occipital lobe. The endoscopic approach provides increased visibility of the surgical field due to the wide-angled panoramic view and is minimally invasive in approaching deep brain lesions compared to the conventional microscopic approach. However, little is known regarding endoscopic OTA for the removal of cerebellar lesions. We experienced a case of a hemangioblastoma in the paramedian superior surface of the cerebellum that was successfully treated with endoscopic OTA combined with gravity retraction while avoiding postoperative visual dysfunction. A 48-year-old woman was diagnosed with a hemangioblastoma in the superior surface of the cerebellum. She underwent tumor removal with endoscopic OTA combined with gravity retraction of the occipital lobe instead of using brain retractors. The narrower space was sufficient for surgical manipulation with a panoramic view obtained by endoscopy. The simultaneous observation of the lesion with both an endoscope and a microscope revealed the superiority of infratentorial visualization with an endoscope. Gross total removal was achieved with no postoperative complications, including visual dysfunction. Endoscopic OTA may reduce the risk of postoperative visual dysfunction because of its minimally invasive nature, which is enhanced when combined with gravity retraction. Additionally, the panoramic view of the endoscope allows favorable visualization of an infratentorial lesion, which is otherwise hidden partly by the tentorium. The use of endoscopy is compatible with OTA, and endoscopic OTA could be an option for superior cerebellar lesions for avoiding visual dysfunction.</p>","PeriodicalId":19260,"journal":{"name":"NMC Case Report Journal","volume":"10 ","pages":"185-189"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ce/de/2188-4226-10-0185.PMC10351956.pdf","citationCount":"0","resultStr":"{\"title\":\"Endoscopic Occipital Transtentorial Approach for Supracerebellar Lesions.\",\"authors\":\"Kento Takahara, Tomoru Miwa, Takashi Iwama, Masahiro Toda\",\"doi\":\"10.2176/jns-nmc.2022-0363\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The occipital transtentorial approach (OTA), which is often applied for superior cerebellar lesions, has an inevitable risk of homonymous hemianopsia due to the retraction of the occipital lobe. The endoscopic approach provides increased visibility of the surgical field due to the wide-angled panoramic view and is minimally invasive in approaching deep brain lesions compared to the conventional microscopic approach. However, little is known regarding endoscopic OTA for the removal of cerebellar lesions. We experienced a case of a hemangioblastoma in the paramedian superior surface of the cerebellum that was successfully treated with endoscopic OTA combined with gravity retraction while avoiding postoperative visual dysfunction. A 48-year-old woman was diagnosed with a hemangioblastoma in the superior surface of the cerebellum. She underwent tumor removal with endoscopic OTA combined with gravity retraction of the occipital lobe instead of using brain retractors. The narrower space was sufficient for surgical manipulation with a panoramic view obtained by endoscopy. The simultaneous observation of the lesion with both an endoscope and a microscope revealed the superiority of infratentorial visualization with an endoscope. Gross total removal was achieved with no postoperative complications, including visual dysfunction. Endoscopic OTA may reduce the risk of postoperative visual dysfunction because of its minimally invasive nature, which is enhanced when combined with gravity retraction. Additionally, the panoramic view of the endoscope allows favorable visualization of an infratentorial lesion, which is otherwise hidden partly by the tentorium. The use of endoscopy is compatible with OTA, and endoscopic OTA could be an option for superior cerebellar lesions for avoiding visual dysfunction.</p>\",\"PeriodicalId\":19260,\"journal\":{\"name\":\"NMC Case Report Journal\",\"volume\":\"10 \",\"pages\":\"185-189\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ce/de/2188-4226-10-0185.PMC10351956.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NMC Case Report Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2176/jns-nmc.2022-0363\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NMC Case Report Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2022-0363","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Endoscopic Occipital Transtentorial Approach for Supracerebellar Lesions.
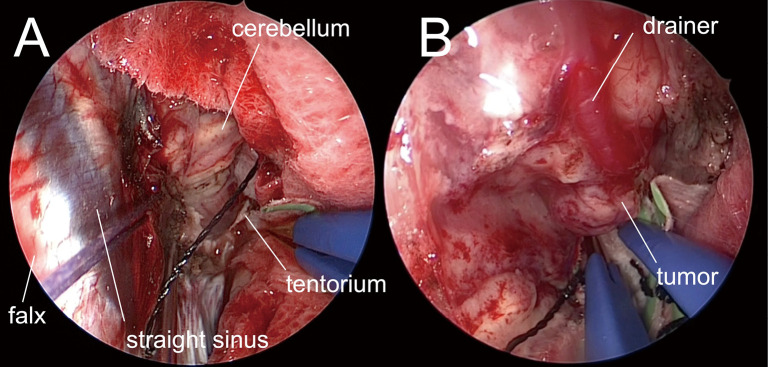
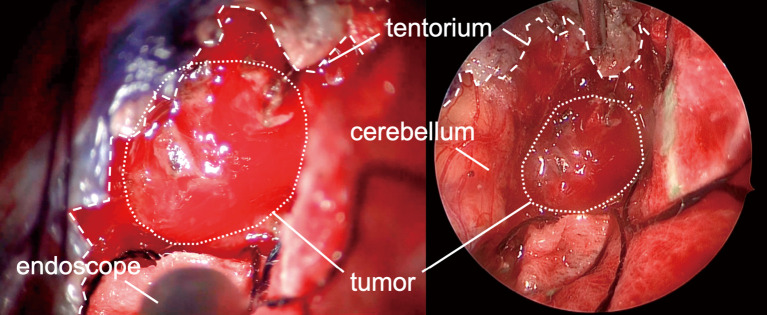
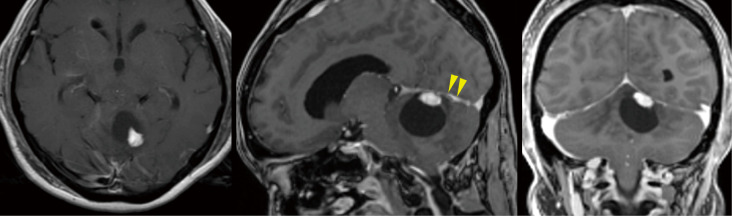
The occipital transtentorial approach (OTA), which is often applied for superior cerebellar lesions, has an inevitable risk of homonymous hemianopsia due to the retraction of the occipital lobe. The endoscopic approach provides increased visibility of the surgical field due to the wide-angled panoramic view and is minimally invasive in approaching deep brain lesions compared to the conventional microscopic approach. However, little is known regarding endoscopic OTA for the removal of cerebellar lesions. We experienced a case of a hemangioblastoma in the paramedian superior surface of the cerebellum that was successfully treated with endoscopic OTA combined with gravity retraction while avoiding postoperative visual dysfunction. A 48-year-old woman was diagnosed with a hemangioblastoma in the superior surface of the cerebellum. She underwent tumor removal with endoscopic OTA combined with gravity retraction of the occipital lobe instead of using brain retractors. The narrower space was sufficient for surgical manipulation with a panoramic view obtained by endoscopy. The simultaneous observation of the lesion with both an endoscope and a microscope revealed the superiority of infratentorial visualization with an endoscope. Gross total removal was achieved with no postoperative complications, including visual dysfunction. Endoscopic OTA may reduce the risk of postoperative visual dysfunction because of its minimally invasive nature, which is enhanced when combined with gravity retraction. Additionally, the panoramic view of the endoscope allows favorable visualization of an infratentorial lesion, which is otherwise hidden partly by the tentorium. The use of endoscopy is compatible with OTA, and endoscopic OTA could be an option for superior cerebellar lesions for avoiding visual dysfunction.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
