{"title":"继发性三叉神经痛:《红旗》的病例报告和文献复习。","authors":"Khawaja Shehryar Nasir, Muhammad Atif Naveed","doi":"10.37029/jcas.v8i1.455","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Trigeminal neuralgia (TN) is characterised by recurrent paroxysmal brief episodes of electric shock-like pain along the trigeminal nerve distribution. Based on the underlying cause, the current classification systems have classified TN into idiopathic, classical and secondary TN. This manuscript presents a case report of a patient seen in the clinic with features of TN secondary to an intracranial lesion.</p><p><strong>Case description: </strong>A 39-year-old female presented to the clinic with a 15-month history of severe, intermittent, short-lasting episodes of pain affecting the left lower teeth, jaw, nose and temporal region. The patient reported familiar shock-like pain during the physical examination when the skin of the left ala of the nose was lightly touched. The rest of the clinical examination was non-significant. The magnetic resonance imaging (MRI) of the brain showed an approximately 20 mm wide lesion at the level of the left cerebellopontine angle. After subsequent tests, the lesion was diagnosed as meningioma, and the patient was treated with stereotactic radiation therapy.</p><p><strong>Practical implications: </strong>In up to 10% of TN cases, the underlying cause can be due to a brain tumour. Although persistent pain, sensory or motor nerve dysfunction, gait disturbances and other neurological signs may concurrently exist, raising a red flag for intracranial pathology, patients often present with pain alone as the heralding symptom of a brain tumour. Due to this, it is imperative that all patients suspected of having TN undergo an MRI of the brain as part of the diagnostic work-up.</p>","PeriodicalId":73631,"journal":{"name":"Journal of cancer & allied specialties","volume":"8 1","pages":"e455"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4f/1d/JCAS-8-455.PMC10166303.pdf","citationCount":"0","resultStr":"{\"title\":\"Secondary Trigeminal Neuralgia: A Case Report and Literature Review of Red Flags.\",\"authors\":\"Khawaja Shehryar Nasir, Muhammad Atif Naveed\",\"doi\":\"10.37029/jcas.v8i1.455\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Trigeminal neuralgia (TN) is characterised by recurrent paroxysmal brief episodes of electric shock-like pain along the trigeminal nerve distribution. Based on the underlying cause, the current classification systems have classified TN into idiopathic, classical and secondary TN. This manuscript presents a case report of a patient seen in the clinic with features of TN secondary to an intracranial lesion.</p><p><strong>Case description: </strong>A 39-year-old female presented to the clinic with a 15-month history of severe, intermittent, short-lasting episodes of pain affecting the left lower teeth, jaw, nose and temporal region. The patient reported familiar shock-like pain during the physical examination when the skin of the left ala of the nose was lightly touched. The rest of the clinical examination was non-significant. The magnetic resonance imaging (MRI) of the brain showed an approximately 20 mm wide lesion at the level of the left cerebellopontine angle. After subsequent tests, the lesion was diagnosed as meningioma, and the patient was treated with stereotactic radiation therapy.</p><p><strong>Practical implications: </strong>In up to 10% of TN cases, the underlying cause can be due to a brain tumour. Although persistent pain, sensory or motor nerve dysfunction, gait disturbances and other neurological signs may concurrently exist, raising a red flag for intracranial pathology, patients often present with pain alone as the heralding symptom of a brain tumour. Due to this, it is imperative that all patients suspected of having TN undergo an MRI of the brain as part of the diagnostic work-up.</p>\",\"PeriodicalId\":73631,\"journal\":{\"name\":\"Journal of cancer & allied specialties\",\"volume\":\"8 1\",\"pages\":\"e455\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-12-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4f/1d/JCAS-8-455.PMC10166303.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of cancer & allied specialties\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.37029/jcas.v8i1.455\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cancer & allied specialties","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.37029/jcas.v8i1.455","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Secondary Trigeminal Neuralgia: A Case Report and Literature Review of Red Flags.
Introduction: Trigeminal neuralgia (TN) is characterised by recurrent paroxysmal brief episodes of electric shock-like pain along the trigeminal nerve distribution. Based on the underlying cause, the current classification systems have classified TN into idiopathic, classical and secondary TN. This manuscript presents a case report of a patient seen in the clinic with features of TN secondary to an intracranial lesion.
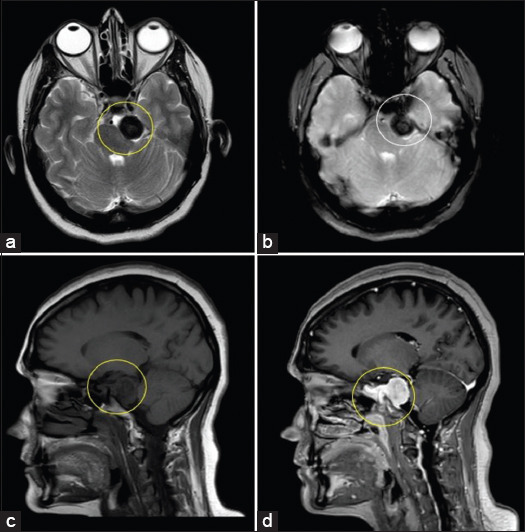
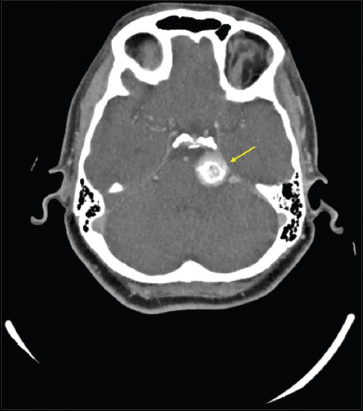
Case description: A 39-year-old female presented to the clinic with a 15-month history of severe, intermittent, short-lasting episodes of pain affecting the left lower teeth, jaw, nose and temporal region. The patient reported familiar shock-like pain during the physical examination when the skin of the left ala of the nose was lightly touched. The rest of the clinical examination was non-significant. The magnetic resonance imaging (MRI) of the brain showed an approximately 20 mm wide lesion at the level of the left cerebellopontine angle. After subsequent tests, the lesion was diagnosed as meningioma, and the patient was treated with stereotactic radiation therapy.
Practical implications: In up to 10% of TN cases, the underlying cause can be due to a brain tumour. Although persistent pain, sensory or motor nerve dysfunction, gait disturbances and other neurological signs may concurrently exist, raising a red flag for intracranial pathology, patients often present with pain alone as the heralding symptom of a brain tumour. Due to this, it is imperative that all patients suspected of having TN undergo an MRI of the brain as part of the diagnostic work-up.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
