Jiafang Wu, Jun Li, Han Chen, Xiuling Shang, Rongguo Yu
{"title":"围手术期中心静脉压的优化与高危手术患者预后的改善有关","authors":"Jiafang Wu, Jun Li, Han Chen, Xiuling Shang, Rongguo Yu","doi":"10.1016/j.jointm.2022.06.003","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>While central venous pressure (CVP) measurement is used to guide fluid management for high-risk surgical patients during the perioperative period, its relationship to patient prognosis is unknown.</p></div><div><h3>Methods</h3><p>This single-center, retrospective observational study enrolled patients undergoing high-risk surgery from February 1, 2014 to November 31, 2020, who were admitted to the surgical intensive care unit (ICU) directly after surgery. Patients were divided into the following three groups according to the first CVP measurement (CVP1) after admission to the ICU: low, CVP1 <8 mmHg; moderate, 8 mmHg≤ CVP1 ≤ 12 mmHg; and high, CVP1 >12 mmHg. Perioperative fluid balance, 28-day mortality, length of stay in the ICU, and hospitalization and surgical complications were compared across groups.</p></div><div><h3>Results</h3><p>Of the 775 high-risk surgical patients enrolled in the study, 228 were included in the analysis. Median (interquartile range) positive fluid balance during surgery was lowest in the low CVP1 group and highest in the high CVP1 group (low CVP1: 770 [410, 1205] mL; moderate CVP1: 1070 [685, 1500] mL; high CVP1: 1570 [1008, 2000] mL; all <em>P</em> <0.001). The volume of positive fluid balance during the perioperative period was correlated with CVP1 (<em>r</em>=0.336, <em>P</em> <0.001). The partial arterial pressure of oxygen(PaO<sub>2</sub>)/fraction of inspired oxygen(FiO<sub>2</sub>) ratio was significantly lower in the high CVP1 group than in the low and moderate CVP1 groups (low CVP1: 400.0 [299.5, 443.3] mmHg; moderate CVP1: 362.5 [330.0, 434.9] mmHg; high CVP1: 335.3 [254.0, 363.5] mmHg; all <em>P</em> <0.001). The incidence of postoperative acute kidney injury (AKI) was lowest in the moderate CVP1 group (low CVP1: 9.2%; moderate CVP1: 2.7%; high CVP1: 16.0%; <em>P</em>=0.007). The proportion of patients receiving renal replacement therapy was highest in the high CVP1 group (low CVP1: 1.5%; moderate CVP1: 0.9%; high CVP1: 10.0%; <em>P</em>=0.014). Logistic regression analysis showed that intraoperative hypotension and CVP1 >12 mmHg were risk factors for AKI within 72 h after surgery (adjusted odds ratio[aOR]=3.875, 95% confidence interval[CI]: 1.378–10.900, <em>P</em>=0.010 and aOR=1.147, 95%CI: 1.006–1.309, <em>P</em>=0.041).</p></div><div><h3>Conclusions</h3><p>CVP that is either too high or too low increases the incidence of postoperative AKI. Sequential fluid therapy based on CVP after patients are transferred to the ICU post-surgery does not reduce the risk of organ dysfunction caused by an excessive amount of intraoperative fluid. However, CVP can be used as a safety limit indicator for perioperative fluid management in high-risk surgical patients.</p></div>","PeriodicalId":73799,"journal":{"name":"Journal of intensive medicine","volume":"3 2","pages":"Pages 165-170"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b2/9d/main.PMC10175704.pdf","citationCount":"0","resultStr":"{\"title\":\"Optimization of central venous pressure during the perioperative period is associated with improved prognosis of high-risk operation patients\",\"authors\":\"Jiafang Wu, Jun Li, Han Chen, Xiuling Shang, Rongguo Yu\",\"doi\":\"10.1016/j.jointm.2022.06.003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>While central venous pressure (CVP) measurement is used to guide fluid management for high-risk surgical patients during the perioperative period, its relationship to patient prognosis is unknown.</p></div><div><h3>Methods</h3><p>This single-center, retrospective observational study enrolled patients undergoing high-risk surgery from February 1, 2014 to November 31, 2020, who were admitted to the surgical intensive care unit (ICU) directly after surgery. Patients were divided into the following three groups according to the first CVP measurement (CVP1) after admission to the ICU: low, CVP1 <8 mmHg; moderate, 8 mmHg≤ CVP1 ≤ 12 mmHg; and high, CVP1 >12 mmHg. Perioperative fluid balance, 28-day mortality, length of stay in the ICU, and hospitalization and surgical complications were compared across groups.</p></div><div><h3>Results</h3><p>Of the 775 high-risk surgical patients enrolled in the study, 228 were included in the analysis. Median (interquartile range) positive fluid balance during surgery was lowest in the low CVP1 group and highest in the high CVP1 group (low CVP1: 770 [410, 1205] mL; moderate CVP1: 1070 [685, 1500] mL; high CVP1: 1570 [1008, 2000] mL; all <em>P</em> <0.001). The volume of positive fluid balance during the perioperative period was correlated with CVP1 (<em>r</em>=0.336, <em>P</em> <0.001). The partial arterial pressure of oxygen(PaO<sub>2</sub>)/fraction of inspired oxygen(FiO<sub>2</sub>) ratio was significantly lower in the high CVP1 group than in the low and moderate CVP1 groups (low CVP1: 400.0 [299.5, 443.3] mmHg; moderate CVP1: 362.5 [330.0, 434.9] mmHg; high CVP1: 335.3 [254.0, 363.5] mmHg; all <em>P</em> <0.001). The incidence of postoperative acute kidney injury (AKI) was lowest in the moderate CVP1 group (low CVP1: 9.2%; moderate CVP1: 2.7%; high CVP1: 16.0%; <em>P</em>=0.007). The proportion of patients receiving renal replacement therapy was highest in the high CVP1 group (low CVP1: 1.5%; moderate CVP1: 0.9%; high CVP1: 10.0%; <em>P</em>=0.014). Logistic regression analysis showed that intraoperative hypotension and CVP1 >12 mmHg were risk factors for AKI within 72 h after surgery (adjusted odds ratio[aOR]=3.875, 95% confidence interval[CI]: 1.378–10.900, <em>P</em>=0.010 and aOR=1.147, 95%CI: 1.006–1.309, <em>P</em>=0.041).</p></div><div><h3>Conclusions</h3><p>CVP that is either too high or too low increases the incidence of postoperative AKI. Sequential fluid therapy based on CVP after patients are transferred to the ICU post-surgery does not reduce the risk of organ dysfunction caused by an excessive amount of intraoperative fluid. However, CVP can be used as a safety limit indicator for perioperative fluid management in high-risk surgical patients.</p></div>\",\"PeriodicalId\":73799,\"journal\":{\"name\":\"Journal of intensive medicine\",\"volume\":\"3 2\",\"pages\":\"Pages 165-170\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-04-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b2/9d/main.PMC10175704.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of intensive medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2667100X22000706\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/8/5 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of intensive medicine","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2667100X22000706","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/8/5 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Optimization of central venous pressure during the perioperative period is associated with improved prognosis of high-risk operation patients
Background
While central venous pressure (CVP) measurement is used to guide fluid management for high-risk surgical patients during the perioperative period, its relationship to patient prognosis is unknown.
Methods
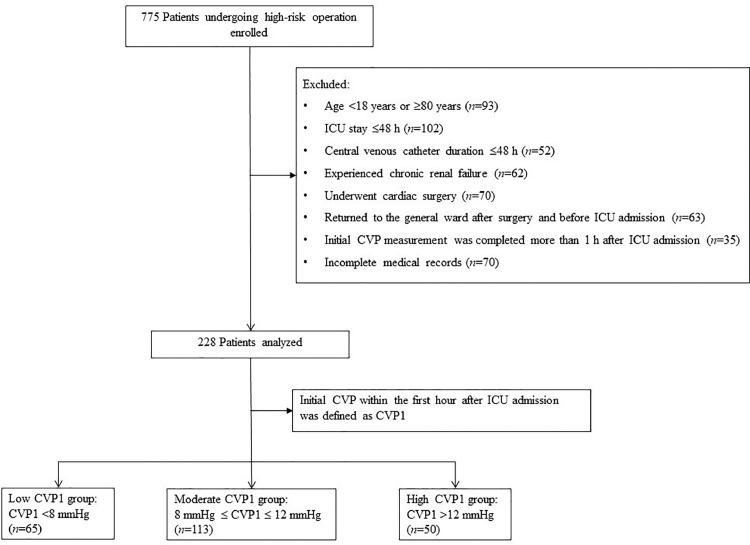
This single-center, retrospective observational study enrolled patients undergoing high-risk surgery from February 1, 2014 to November 31, 2020, who were admitted to the surgical intensive care unit (ICU) directly after surgery. Patients were divided into the following three groups according to the first CVP measurement (CVP1) after admission to the ICU: low, CVP1 <8 mmHg; moderate, 8 mmHg≤ CVP1 ≤ 12 mmHg; and high, CVP1 >12 mmHg. Perioperative fluid balance, 28-day mortality, length of stay in the ICU, and hospitalization and surgical complications were compared across groups.
Results
Of the 775 high-risk surgical patients enrolled in the study, 228 were included in the analysis. Median (interquartile range) positive fluid balance during surgery was lowest in the low CVP1 group and highest in the high CVP1 group (low CVP1: 770 [410, 1205] mL; moderate CVP1: 1070 [685, 1500] mL; high CVP1: 1570 [1008, 2000] mL; all P <0.001). The volume of positive fluid balance during the perioperative period was correlated with CVP1 (r=0.336, P <0.001). The partial arterial pressure of oxygen(PaO2)/fraction of inspired oxygen(FiO2) ratio was significantly lower in the high CVP1 group than in the low and moderate CVP1 groups (low CVP1: 400.0 [299.5, 443.3] mmHg; moderate CVP1: 362.5 [330.0, 434.9] mmHg; high CVP1: 335.3 [254.0, 363.5] mmHg; all P <0.001). The incidence of postoperative acute kidney injury (AKI) was lowest in the moderate CVP1 group (low CVP1: 9.2%; moderate CVP1: 2.7%; high CVP1: 16.0%; P=0.007). The proportion of patients receiving renal replacement therapy was highest in the high CVP1 group (low CVP1: 1.5%; moderate CVP1: 0.9%; high CVP1: 10.0%; P=0.014). Logistic regression analysis showed that intraoperative hypotension and CVP1 >12 mmHg were risk factors for AKI within 72 h after surgery (adjusted odds ratio[aOR]=3.875, 95% confidence interval[CI]: 1.378–10.900, P=0.010 and aOR=1.147, 95%CI: 1.006–1.309, P=0.041).
Conclusions
CVP that is either too high or too low increases the incidence of postoperative AKI. Sequential fluid therapy based on CVP after patients are transferred to the ICU post-surgery does not reduce the risk of organ dysfunction caused by an excessive amount of intraoperative fluid. However, CVP can be used as a safety limit indicator for perioperative fluid management in high-risk surgical patients.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
