Catherina Lück, Gernot Beutel, W Nikolaus Kühn-Velten, Jan T Kielstein
{"title":"接受间歇性血液透析和长期间歇性肾脏替代疗法的急性肾损伤患者的单剂量药代动力学和环磷酰胺总清除率:病例报告。","authors":"Catherina Lück, Gernot Beutel, W Nikolaus Kühn-Velten, Jan T Kielstein","doi":"10.1159/000531129","DOIUrl":null,"url":null,"abstract":"<p><p>The largest study on cyclophosphamide pharmacokinetics in dialysis patients comprises of 6 subjects. In the 2 decades since these data were obtained, dialyser membranes, treatment intensities, and treatment duration have changed considerably making new pharmacokinetic studies desirable. We aimed to readdress the pharmacokinetics of cyclophosphamide in a 74-year-old critically ill male suffering from ANCA-associated vasculitis. Due to an acute-on-chronic kidney injury, he underwent intermittent (IHD) and prolonged intermittent kidney replacement therapy (PIKRT). IHD was started 7 h after end of a cyclophosphamide infusion with a blood/dialysate flow of 300 mL/min for 255 min, followed by PIKRT with a blood/dialysate flow of 140 mL/min for 540 min, both using a 1.3 m<sup>2</sup> polysulphone high-flux dialyser (F60S, Fresenius Medical Care). Peak concentration of cyclophosphamide was 20.2 mg/L. Using IHD and PIKRT serum concentration of cyclophosphamide decreased to 1.2 mg/L after IHD and to <0.1 mg/L after PIKRT with dialyser-clearances of 153.0 mL/min and 84.9 mL/min, respectively. Total recovery of cyclophosphamide, calculated from the collected dialysate, was 57.5 mg (7.7% of administered dose) for IHD and was 8.3 mg (1.1% of administered dose) for PIKRT. By using IHD with a high-flux dialyser cyclophosphamide could be eliminated. Remaining cyclophosphamide should be eliminated by PIKRT. Hence, even in the absence of renal function a dose >50% of the recommended for patient with normal renal function may be applied, as complete elimination of the parent drug by modern dialysis is feasible.</p>","PeriodicalId":9599,"journal":{"name":"Case Reports in Nephrology and Dialysis","volume":"13 1","pages":"70-74"},"PeriodicalIF":0.9000,"publicationDate":"2023-07-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/06/5f/cnd-2023-0013-0001-531129.PMC10359690.pdf","citationCount":"0","resultStr":"{\"title\":\"Single-Dose Pharmacokinetics and Total Removal of Cyclophosphamide in a Patient with Acute Kidney Injury Undergoing Intermittent Haemodialysis and Prolonged Intermittent Kidney Replacement Therapy: A Case Report.\",\"authors\":\"Catherina Lück, Gernot Beutel, W Nikolaus Kühn-Velten, Jan T Kielstein\",\"doi\":\"10.1159/000531129\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The largest study on cyclophosphamide pharmacokinetics in dialysis patients comprises of 6 subjects. In the 2 decades since these data were obtained, dialyser membranes, treatment intensities, and treatment duration have changed considerably making new pharmacokinetic studies desirable. We aimed to readdress the pharmacokinetics of cyclophosphamide in a 74-year-old critically ill male suffering from ANCA-associated vasculitis. Due to an acute-on-chronic kidney injury, he underwent intermittent (IHD) and prolonged intermittent kidney replacement therapy (PIKRT). IHD was started 7 h after end of a cyclophosphamide infusion with a blood/dialysate flow of 300 mL/min for 255 min, followed by PIKRT with a blood/dialysate flow of 140 mL/min for 540 min, both using a 1.3 m<sup>2</sup> polysulphone high-flux dialyser (F60S, Fresenius Medical Care). Peak concentration of cyclophosphamide was 20.2 mg/L. Using IHD and PIKRT serum concentration of cyclophosphamide decreased to 1.2 mg/L after IHD and to <0.1 mg/L after PIKRT with dialyser-clearances of 153.0 mL/min and 84.9 mL/min, respectively. Total recovery of cyclophosphamide, calculated from the collected dialysate, was 57.5 mg (7.7% of administered dose) for IHD and was 8.3 mg (1.1% of administered dose) for PIKRT. By using IHD with a high-flux dialyser cyclophosphamide could be eliminated. Remaining cyclophosphamide should be eliminated by PIKRT. Hence, even in the absence of renal function a dose >50% of the recommended for patient with normal renal function may be applied, as complete elimination of the parent drug by modern dialysis is feasible.</p>\",\"PeriodicalId\":9599,\"journal\":{\"name\":\"Case Reports in Nephrology and Dialysis\",\"volume\":\"13 1\",\"pages\":\"70-74\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2023-07-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/06/5f/cnd-2023-0013-0001-531129.PMC10359690.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Nephrology and Dialysis\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000531129\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Nephrology and Dialysis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000531129","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
关于透析患者环磷酰胺药代动力学的最大规模研究包括 6 个受试者。在获得这些数据后的 20 年中,透析器膜、治疗强度和治疗持续时间都发生了很大变化,因此需要进行新的药代动力学研究。我们的目的是重新研究一名 74 岁男性 ANCA 相关性血管炎重症患者的环磷酰胺药代动力学。由于急性慢性肾损伤,他接受了间歇性(IHD)和长期间歇性肾替代治疗(PIKRT)。IHD在环磷酰胺输注结束7小时后开始,血液/透析液流量为300毫升/分钟,持续255分钟,随后进行PIKRT,血液/透析液流量为140毫升/分钟,持续540分钟,均使用1.3平方米的多聚砜高通量透析器(F60S,费森尤斯医疗用品公司)。环磷酰胺的峰值浓度为20.2毫克/升。使用IHD和PIKRT后,环磷酰胺的血清浓度降至1.2毫克/升,可应用于肾功能正常患者的建议浓度的50%,因为通过现代透析完全清除母体药物是可行的。
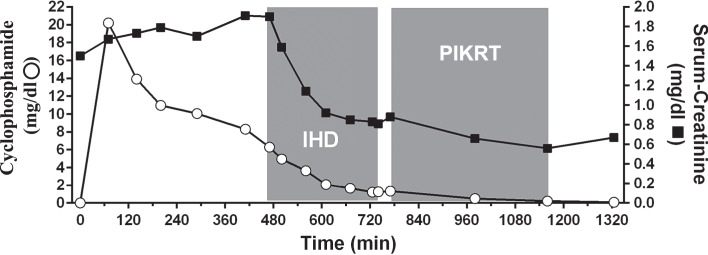
Single-Dose Pharmacokinetics and Total Removal of Cyclophosphamide in a Patient with Acute Kidney Injury Undergoing Intermittent Haemodialysis and Prolonged Intermittent Kidney Replacement Therapy: A Case Report.
The largest study on cyclophosphamide pharmacokinetics in dialysis patients comprises of 6 subjects. In the 2 decades since these data were obtained, dialyser membranes, treatment intensities, and treatment duration have changed considerably making new pharmacokinetic studies desirable. We aimed to readdress the pharmacokinetics of cyclophosphamide in a 74-year-old critically ill male suffering from ANCA-associated vasculitis. Due to an acute-on-chronic kidney injury, he underwent intermittent (IHD) and prolonged intermittent kidney replacement therapy (PIKRT). IHD was started 7 h after end of a cyclophosphamide infusion with a blood/dialysate flow of 300 mL/min for 255 min, followed by PIKRT with a blood/dialysate flow of 140 mL/min for 540 min, both using a 1.3 m2 polysulphone high-flux dialyser (F60S, Fresenius Medical Care). Peak concentration of cyclophosphamide was 20.2 mg/L. Using IHD and PIKRT serum concentration of cyclophosphamide decreased to 1.2 mg/L after IHD and to <0.1 mg/L after PIKRT with dialyser-clearances of 153.0 mL/min and 84.9 mL/min, respectively. Total recovery of cyclophosphamide, calculated from the collected dialysate, was 57.5 mg (7.7% of administered dose) for IHD and was 8.3 mg (1.1% of administered dose) for PIKRT. By using IHD with a high-flux dialyser cyclophosphamide could be eliminated. Remaining cyclophosphamide should be eliminated by PIKRT. Hence, even in the absence of renal function a dose >50% of the recommended for patient with normal renal function may be applied, as complete elimination of the parent drug by modern dialysis is feasible.
期刊介绍:
This peer-reviewed online-only journal publishes original case reports covering the entire spectrum of nephrology and dialysis, including genetic susceptibility, clinical presentation, diagnosis, treatment or prevention, toxicities of therapy, critical care, supportive care, quality-of-life and survival issues. The journal will also accept case reports dealing with the use of novel technologies, both in the arena of diagnosis and treatment. Supplementary material is welcomed.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
