{"title":"子宫动脉栓塞治疗产后出血后子宫坏死的子宫切除术备用管理。","authors":"Myriam Chlela, Josette Dawkins, Gregory Lewis","doi":"10.1155/2023/8276110","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Postpartum hemorrhage (PPH) is one of the leading causes of maternal morbidity and mortality. Uterine artery embolization (UAE) is an effective procedural intervention for controlling PPH. Uterine necrosis (UN) is a rare complication of UAE and its management usually results in hysterectomy. We highlight a case of UAE complicated by UN managed conservatively without hysterectomy.</p><p><strong>Case: </strong>This is the case of a 30-year-old patient who had a cesarean section delivery and subsequently developed PPH due to uterine atony. The estimated blood loss (EBL) was 2500 ml; despite the use of uterotonic medications and trial of intrauterine balloon tamponade. She successfully underwent a UAE with no immediate complications. The remainder of her postnatal course was uncomplicated, and she was discharged on postoperative day 4. On postoperative day 28, the patient presented with fever, vaginal discharge, and abdominal pain. An abdomino-pelvic computed tomography scan revealed areas of necrosis within the uterus secondary to recent UAE. After minimal clinical improvement, the patient underwent a dilation and curettage with ultrasound guidance. The patient improved clinically and was discharged home to complete a 14-day course of antibiotics.</p><p><strong>Conclusion: </strong>UAE is an important minimally invasive approach to the management of PPH. UN following UAE can present a clinical challenge to physicians, with the underlying pathophysiology being use of small embolizing particles during UAE and lack of arterial collaterals to embolized areas. A total of 19 cases of UN post-UAE have been described of which most of these cases were managed with a hysterectomy. In this case, an alternative treatment plan was successfully implemented via dilation and curettage under ultrasound guidance for removal of organized necrotic tissue. This was sufficient to improve the patient's symptoms and clinical outcome and saved the patient from the morbidity and mortality risks associated with a hysterectomy.</p>","PeriodicalId":9610,"journal":{"name":"Case Reports in Obstetrics and Gynecology","volume":"2023 ","pages":"8276110"},"PeriodicalIF":0.8000,"publicationDate":"2023-07-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10372334/pdf/","citationCount":"0","resultStr":"{\"title\":\"Hysterectomy Sparing Management of Uterine Necrosis following Uterine Artery Embolization for Postpartum Hemorrhage.\",\"authors\":\"Myriam Chlela, Josette Dawkins, Gregory Lewis\",\"doi\":\"10.1155/2023/8276110\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Postpartum hemorrhage (PPH) is one of the leading causes of maternal morbidity and mortality. Uterine artery embolization (UAE) is an effective procedural intervention for controlling PPH. Uterine necrosis (UN) is a rare complication of UAE and its management usually results in hysterectomy. We highlight a case of UAE complicated by UN managed conservatively without hysterectomy.</p><p><strong>Case: </strong>This is the case of a 30-year-old patient who had a cesarean section delivery and subsequently developed PPH due to uterine atony. The estimated blood loss (EBL) was 2500 ml; despite the use of uterotonic medications and trial of intrauterine balloon tamponade. She successfully underwent a UAE with no immediate complications. The remainder of her postnatal course was uncomplicated, and she was discharged on postoperative day 4. On postoperative day 28, the patient presented with fever, vaginal discharge, and abdominal pain. An abdomino-pelvic computed tomography scan revealed areas of necrosis within the uterus secondary to recent UAE. After minimal clinical improvement, the patient underwent a dilation and curettage with ultrasound guidance. The patient improved clinically and was discharged home to complete a 14-day course of antibiotics.</p><p><strong>Conclusion: </strong>UAE is an important minimally invasive approach to the management of PPH. UN following UAE can present a clinical challenge to physicians, with the underlying pathophysiology being use of small embolizing particles during UAE and lack of arterial collaterals to embolized areas. A total of 19 cases of UN post-UAE have been described of which most of these cases were managed with a hysterectomy. In this case, an alternative treatment plan was successfully implemented via dilation and curettage under ultrasound guidance for removal of organized necrotic tissue. This was sufficient to improve the patient's symptoms and clinical outcome and saved the patient from the morbidity and mortality risks associated with a hysterectomy.</p>\",\"PeriodicalId\":9610,\"journal\":{\"name\":\"Case Reports in Obstetrics and Gynecology\",\"volume\":\"2023 \",\"pages\":\"8276110\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2023-07-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10372334/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Obstetrics and Gynecology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2023/8276110\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Obstetrics and Gynecology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/8276110","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Hysterectomy Sparing Management of Uterine Necrosis following Uterine Artery Embolization for Postpartum Hemorrhage.
Background: Postpartum hemorrhage (PPH) is one of the leading causes of maternal morbidity and mortality. Uterine artery embolization (UAE) is an effective procedural intervention for controlling PPH. Uterine necrosis (UN) is a rare complication of UAE and its management usually results in hysterectomy. We highlight a case of UAE complicated by UN managed conservatively without hysterectomy.
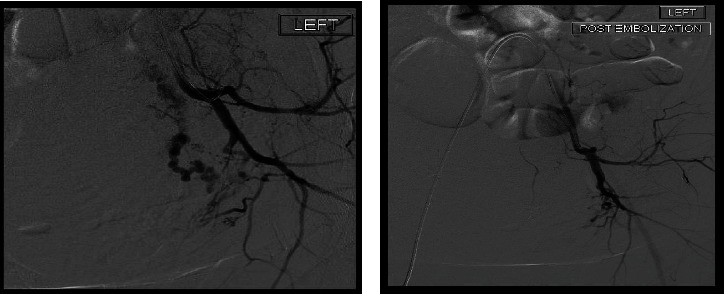
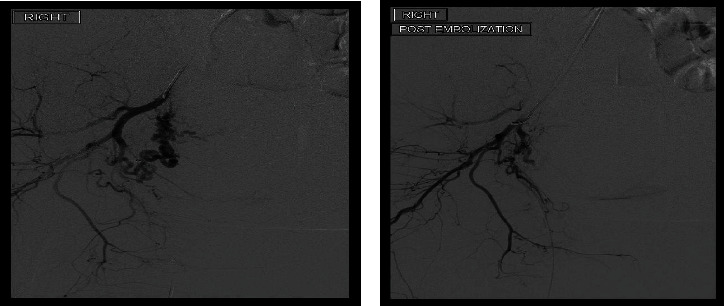
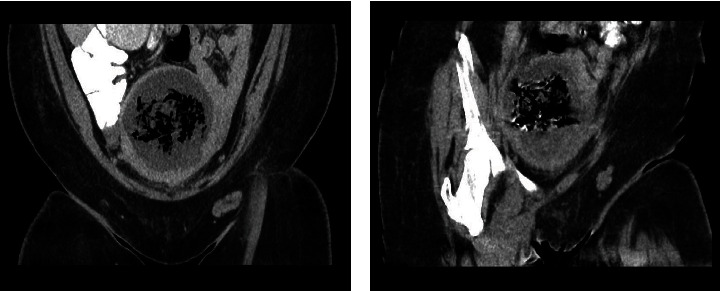
Case: This is the case of a 30-year-old patient who had a cesarean section delivery and subsequently developed PPH due to uterine atony. The estimated blood loss (EBL) was 2500 ml; despite the use of uterotonic medications and trial of intrauterine balloon tamponade. She successfully underwent a UAE with no immediate complications. The remainder of her postnatal course was uncomplicated, and she was discharged on postoperative day 4. On postoperative day 28, the patient presented with fever, vaginal discharge, and abdominal pain. An abdomino-pelvic computed tomography scan revealed areas of necrosis within the uterus secondary to recent UAE. After minimal clinical improvement, the patient underwent a dilation and curettage with ultrasound guidance. The patient improved clinically and was discharged home to complete a 14-day course of antibiotics.
Conclusion: UAE is an important minimally invasive approach to the management of PPH. UN following UAE can present a clinical challenge to physicians, with the underlying pathophysiology being use of small embolizing particles during UAE and lack of arterial collaterals to embolized areas. A total of 19 cases of UN post-UAE have been described of which most of these cases were managed with a hysterectomy. In this case, an alternative treatment plan was successfully implemented via dilation and curettage under ultrasound guidance for removal of organized necrotic tissue. This was sufficient to improve the patient's symptoms and clinical outcome and saved the patient from the morbidity and mortality risks associated with a hysterectomy.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
