Priya Vart, Jawad H Butt, Niels Jongs, Meir Schechter, Glenn M Chertow, David C Wheeler, Roberto Pecoits-Filho, Anna Maria Langkilde, Ricardo Correa-Rotter, Peter Rossing, John J V McMurray, Hiddo J L Heerspink
{"title":"达帕格列净对不同虚弱程度的慢性肾病患者的疗效和安全性","authors":"Priya Vart, Jawad H Butt, Niels Jongs, Meir Schechter, Glenn M Chertow, David C Wheeler, Roberto Pecoits-Filho, Anna Maria Langkilde, Ricardo Correa-Rotter, Peter Rossing, John J V McMurray, Hiddo J L Heerspink","doi":"10.1093/gerona/glad181","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A sizeable proportion of patients with chronic kidney disease (CKD) are reported to be frail. Here we examined the safety and efficacy of dapagliflozin in patients with CKD by frailty level.</p><p><strong>Methods: </strong>Adults with CKD, with/without type 2 diabetes, with an estimated glomerular filtration rate (eGFR) of 25-75 mL/min/1.73 m2, and urinary albumin-to-creatinine ratio 200-5 000 mg/g were randomized to dapagliflozin (10 mg/day) or placebo. The primary endpoint was a composite of sustained ≥50% eGFR decline, end-stage kidney disease (ESKD), or death from kidney or cardiovascular (CV) causes.</p><p><strong>Results: </strong>Frailty index (FI), assessed by Rockwood cumulative deficit approach, was calculable in 4 303/4 304 (99.9%) patients: 1 162 (27.0%) in not-to-mildly frail (FI ≤0.210), 1 642 (38.2%) in moderately frail (FI 0.211-0.310), and 1 499 (34.8%) in severely frail categories (FI >0.311). Dapagliflozin reduced the risk of the primary composite endpoint across all FI categories (hazard ratios [95% confidence interval {CI}]: 0.50 [0.33-0.76], 0.62 [0.45-0.85], and 0.64 [0.49--0.83], respectively; p-interaction = 0.67). Results were similar for secondary outcomes including kidney composite outcome (sustained ≥50% eGFR decline, ESKD or death from kidney cause; p-interaction = 0.44), CV endpoint (heart failure hospitalization or CV death; p-interaction = 0.63), and all-cause mortality (p-interaction p = .42). Results were consistent when using FI as a continuous variable. Occurrence of serious adverse events was numerically lower in patients receiving dapagliflozin versus placebo in all FI categories (16.9% vs 20.1%, 26.3% vs 30.7%, and 42.9% vs 47.8%, in not-to-mildly, moderately, and severely frail categories, respectively).</p><p><strong>Conclusions: </strong>The relative benefit of dapagliflozin for all outcomes was consistent across all frailty categories, with no difference in associated safety.</p>","PeriodicalId":49953,"journal":{"name":"Journals of Gerontology Series A-Biological Sciences and Medical Sciences","volume":" ","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2024-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10809037/pdf/","citationCount":"0","resultStr":"{\"title\":\"Efficacy and Safety of Dapagliflozin in Patients With Chronic Kidney Disease Across the Spectrum of Frailty.\",\"authors\":\"Priya Vart, Jawad H Butt, Niels Jongs, Meir Schechter, Glenn M Chertow, David C Wheeler, Roberto Pecoits-Filho, Anna Maria Langkilde, Ricardo Correa-Rotter, Peter Rossing, John J V McMurray, Hiddo J L Heerspink\",\"doi\":\"10.1093/gerona/glad181\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A sizeable proportion of patients with chronic kidney disease (CKD) are reported to be frail. Here we examined the safety and efficacy of dapagliflozin in patients with CKD by frailty level.</p><p><strong>Methods: </strong>Adults with CKD, with/without type 2 diabetes, with an estimated glomerular filtration rate (eGFR) of 25-75 mL/min/1.73 m2, and urinary albumin-to-creatinine ratio 200-5 000 mg/g were randomized to dapagliflozin (10 mg/day) or placebo. The primary endpoint was a composite of sustained ≥50% eGFR decline, end-stage kidney disease (ESKD), or death from kidney or cardiovascular (CV) causes.</p><p><strong>Results: </strong>Frailty index (FI), assessed by Rockwood cumulative deficit approach, was calculable in 4 303/4 304 (99.9%) patients: 1 162 (27.0%) in not-to-mildly frail (FI ≤0.210), 1 642 (38.2%) in moderately frail (FI 0.211-0.310), and 1 499 (34.8%) in severely frail categories (FI >0.311). Dapagliflozin reduced the risk of the primary composite endpoint across all FI categories (hazard ratios [95% confidence interval {CI}]: 0.50 [0.33-0.76], 0.62 [0.45-0.85], and 0.64 [0.49--0.83], respectively; p-interaction = 0.67). Results were similar for secondary outcomes including kidney composite outcome (sustained ≥50% eGFR decline, ESKD or death from kidney cause; p-interaction = 0.44), CV endpoint (heart failure hospitalization or CV death; p-interaction = 0.63), and all-cause mortality (p-interaction p = .42). Results were consistent when using FI as a continuous variable. Occurrence of serious adverse events was numerically lower in patients receiving dapagliflozin versus placebo in all FI categories (16.9% vs 20.1%, 26.3% vs 30.7%, and 42.9% vs 47.8%, in not-to-mildly, moderately, and severely frail categories, respectively).</p><p><strong>Conclusions: </strong>The relative benefit of dapagliflozin for all outcomes was consistent across all frailty categories, with no difference in associated safety.</p>\",\"PeriodicalId\":49953,\"journal\":{\"name\":\"Journals of Gerontology Series A-Biological Sciences and Medical Sciences\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2024-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10809037/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journals of Gerontology Series A-Biological Sciences and Medical Sciences\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/gerona/glad181\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journals of Gerontology Series A-Biological Sciences and Medical Sciences","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/gerona/glad181","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:据报道,相当一部分慢性肾脏病(CKD)患者体质虚弱。在此,我们根据虚弱程度研究了达帕格列净对 CKD 患者的安全性和有效性:方法:将伴有/不伴有2型糖尿病、估计肾小球滤过率(eGFR)为25-75 mL/min/1.73 m2、尿白蛋白与肌酐比值为200-5 000 mg/g的成人CKD患者随机分为达帕格列净(10 mg/天)或安慰剂。主要终点是eGFR持续下降≥50%、终末期肾病(ESKD)或因肾脏或心血管(CV)原因死亡的复合终点:4 303/4 304(99.9%)名患者的虚弱指数(FI)可通过罗克伍德累积亏损法进行评估,1 162(27.0%)名患者的虚弱指数可通过罗克伍德累积亏损法进行评估:其中 1 162 人(27.0%)属于非轻度虚弱(FI ≤0.210),1 642 人(38.2%)属于中度虚弱(FI 0.211-0.310),1 499 人(34.8%)属于重度虚弱(FI >0.311)。Dapagliflozin降低了所有FI类别的主要复合终点风险(危险比[95%置信区间{CI}]:0.50[0.33-0.310]):分别为 0.50 [0.33-0.76]、0.62 [0.45-0.85] 和 0.64 [0.49--0.83];p-交互作用 = 0.67)。肾脏综合结局(eGFR 持续下降≥50%、ESKD 或肾脏原因导致的死亡;p-交互作用 = 0.44)、CV 终点(心力衰竭住院或 CV 死亡;p-交互作用 = 0.63)和全因死亡率(p-交互作用 p = 0.42)等次要结局的结果相似。将 FI 作为连续变量时,结果是一致的。在所有FI类别中,接受达帕格列净治疗的患者严重不良事件发生率均低于安慰剂(在非轻度、中度和重度虚弱类别中,严重不良事件发生率分别为16.9% vs 20.1%、26.3% vs 30.7%和42.9% vs 47.8%):在所有虚弱类别中,达帕格列净对所有结果的相对获益是一致的,相关安全性没有差异。
Efficacy and Safety of Dapagliflozin in Patients With Chronic Kidney Disease Across the Spectrum of Frailty.
Background: A sizeable proportion of patients with chronic kidney disease (CKD) are reported to be frail. Here we examined the safety and efficacy of dapagliflozin in patients with CKD by frailty level.
Methods: Adults with CKD, with/without type 2 diabetes, with an estimated glomerular filtration rate (eGFR) of 25-75 mL/min/1.73 m2, and urinary albumin-to-creatinine ratio 200-5 000 mg/g were randomized to dapagliflozin (10 mg/day) or placebo. The primary endpoint was a composite of sustained ≥50% eGFR decline, end-stage kidney disease (ESKD), or death from kidney or cardiovascular (CV) causes.
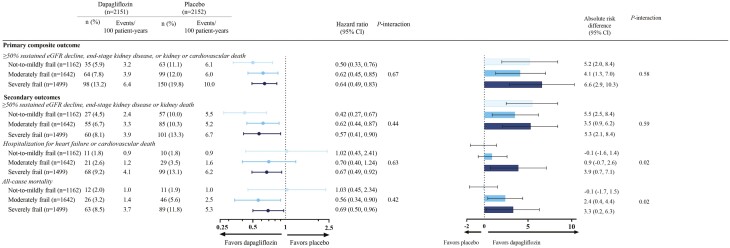
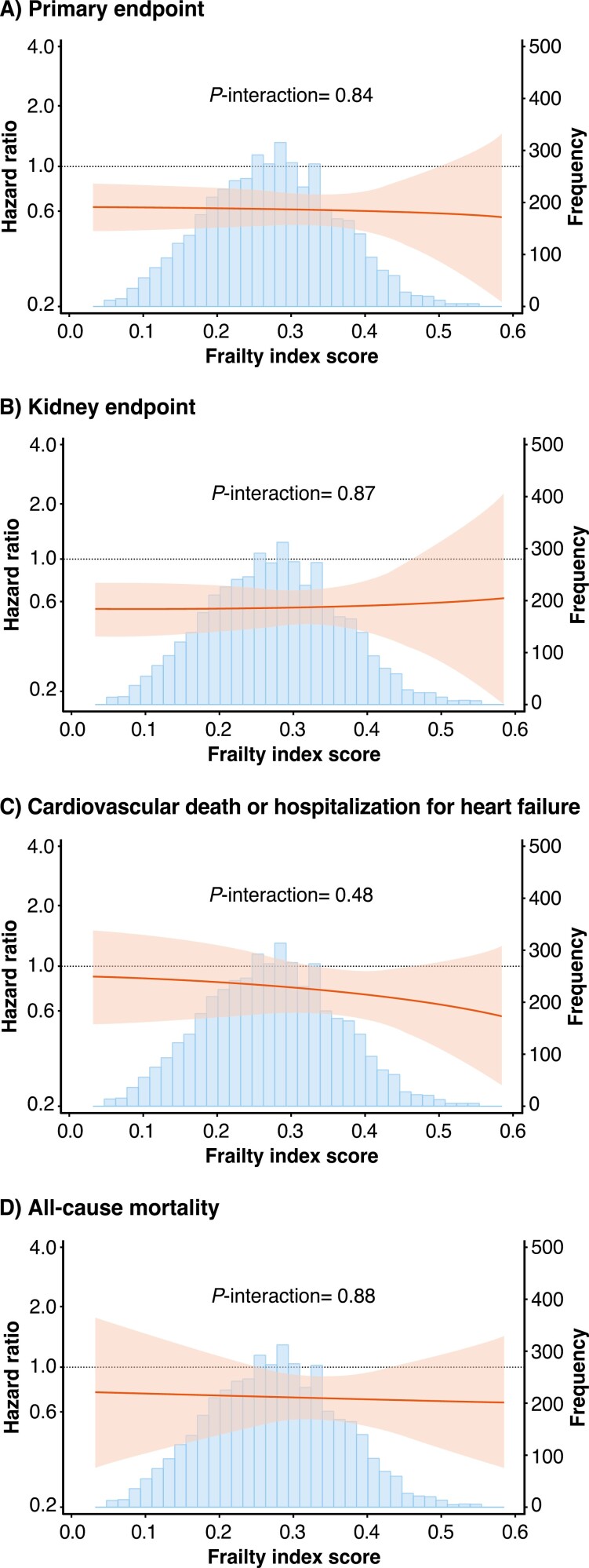
Results: Frailty index (FI), assessed by Rockwood cumulative deficit approach, was calculable in 4 303/4 304 (99.9%) patients: 1 162 (27.0%) in not-to-mildly frail (FI ≤0.210), 1 642 (38.2%) in moderately frail (FI 0.211-0.310), and 1 499 (34.8%) in severely frail categories (FI >0.311). Dapagliflozin reduced the risk of the primary composite endpoint across all FI categories (hazard ratios [95% confidence interval {CI}]: 0.50 [0.33-0.76], 0.62 [0.45-0.85], and 0.64 [0.49--0.83], respectively; p-interaction = 0.67). Results were similar for secondary outcomes including kidney composite outcome (sustained ≥50% eGFR decline, ESKD or death from kidney cause; p-interaction = 0.44), CV endpoint (heart failure hospitalization or CV death; p-interaction = 0.63), and all-cause mortality (p-interaction p = .42). Results were consistent when using FI as a continuous variable. Occurrence of serious adverse events was numerically lower in patients receiving dapagliflozin versus placebo in all FI categories (16.9% vs 20.1%, 26.3% vs 30.7%, and 42.9% vs 47.8%, in not-to-mildly, moderately, and severely frail categories, respectively).
Conclusions: The relative benefit of dapagliflozin for all outcomes was consistent across all frailty categories, with no difference in associated safety.
期刊介绍:
Publishes articles representing the full range of medical sciences pertaining to aging. Appropriate areas include, but are not limited to, basic medical science, clinical epidemiology, clinical research, and health services research for professions such as medicine, dentistry, allied health sciences, and nursing. It publishes articles on research pertinent to human biology and disease.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
