{"title":"成人先天性膈疝伴胃穿孔:胸内胃穿孔。","authors":"Mehmet Taner Ünlü, Serkan Sarı, Ozan Çalışkan","doi":"10.14744/tjtes.2022.62289","DOIUrl":null,"url":null,"abstract":"<p><p>Congenital diaphragmatic hernias are rarely seen and they are usually diagnosed in the neonatal period. Congenital diaphragmatic de-fect, also known as Bochdalek hernia, usually occurs with the persistence of the pleuroperitoneal canal in the left posterolateral region of the diaphragm in the embryological period. Although it is rarely seen in the adults, conditions such as intestinal volvulus, strangulation, or perforation with congenital diaphragm defect progress with high mortality and morbidity. In this study, we reported our case that we operated for intrathoracic gastric perforation with congenital diaphragmatic defect. When the patient admitted to the hospital, he had an atypical abdominal pain, significant back pain, and suspicious respiratory complaints. Radiological imaging showed that the stomach and the spleen were located in the left hemithorax due to diaphragmatic hernia also stomach was very dilated. Tachycardia, hypotension, and low saturation developed on the 2nd day of the patient's hospitalization. In the control imaging of the patient, in the left hemithorax, stomach was collapsed and the surrounding appearance compatible with hydropneumothorax, after that findings emergency laparotomy was decided. During the operation, as demonstrated by the radiological findings, a diaphragm defect was seen in the left posterolateral region of the diaphragm. The stomach and spleen were herniated to the left hemithorax from this defect. The stomach and spleen were reduced into the abdomen. The left hemithorax was lavaged with 2000 cc isotonic, left tube thoracostomy was applied, and the diaphragm was repaired. The anterior stomach was primarily repaired. In post-operative follow-up, there were no complications other than wound infection and thoracic tube of the patient was removed. The patient who tolerated enteral food was discharged from hospital with full recovery.</p>","PeriodicalId":49398,"journal":{"name":"Ulusal Travma Ve Acil Cerrahi Dergisi-Turkish Journal of Trauma & Emergency Surgery","volume":"29 4","pages":"538-542"},"PeriodicalIF":0.8000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6d/ba/TJTES-29-538.PMC10214891.pdf","citationCount":"0","resultStr":"{\"title\":\"Congenital diaphragmatic hernia with gastric perforation in adult: Intrathoracic gastric perforation.\",\"authors\":\"Mehmet Taner Ünlü, Serkan Sarı, Ozan Çalışkan\",\"doi\":\"10.14744/tjtes.2022.62289\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Congenital diaphragmatic hernias are rarely seen and they are usually diagnosed in the neonatal period. Congenital diaphragmatic de-fect, also known as Bochdalek hernia, usually occurs with the persistence of the pleuroperitoneal canal in the left posterolateral region of the diaphragm in the embryological period. Although it is rarely seen in the adults, conditions such as intestinal volvulus, strangulation, or perforation with congenital diaphragm defect progress with high mortality and morbidity. In this study, we reported our case that we operated for intrathoracic gastric perforation with congenital diaphragmatic defect. When the patient admitted to the hospital, he had an atypical abdominal pain, significant back pain, and suspicious respiratory complaints. Radiological imaging showed that the stomach and the spleen were located in the left hemithorax due to diaphragmatic hernia also stomach was very dilated. Tachycardia, hypotension, and low saturation developed on the 2nd day of the patient's hospitalization. In the control imaging of the patient, in the left hemithorax, stomach was collapsed and the surrounding appearance compatible with hydropneumothorax, after that findings emergency laparotomy was decided. During the operation, as demonstrated by the radiological findings, a diaphragm defect was seen in the left posterolateral region of the diaphragm. The stomach and spleen were herniated to the left hemithorax from this defect. The stomach and spleen were reduced into the abdomen. The left hemithorax was lavaged with 2000 cc isotonic, left tube thoracostomy was applied, and the diaphragm was repaired. The anterior stomach was primarily repaired. In post-operative follow-up, there were no complications other than wound infection and thoracic tube of the patient was removed. The patient who tolerated enteral food was discharged from hospital with full recovery.</p>\",\"PeriodicalId\":49398,\"journal\":{\"name\":\"Ulusal Travma Ve Acil Cerrahi Dergisi-Turkish Journal of Trauma & Emergency Surgery\",\"volume\":\"29 4\",\"pages\":\"538-542\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2023-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6d/ba/TJTES-29-538.PMC10214891.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Ulusal Travma Ve Acil Cerrahi Dergisi-Turkish Journal of Trauma & Emergency Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.14744/tjtes.2022.62289\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ulusal Travma Ve Acil Cerrahi Dergisi-Turkish Journal of Trauma & Emergency Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14744/tjtes.2022.62289","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Congenital diaphragmatic hernia with gastric perforation in adult: Intrathoracic gastric perforation.
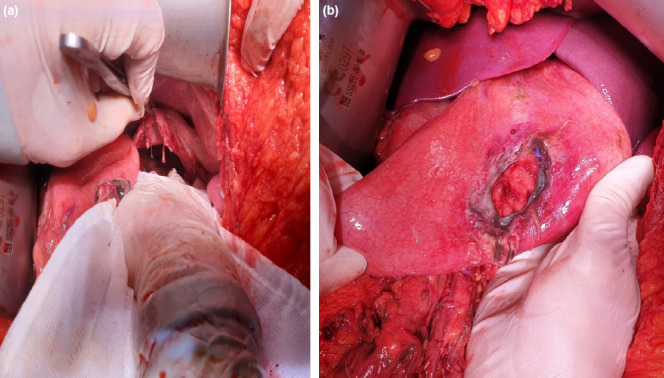
Congenital diaphragmatic hernias are rarely seen and they are usually diagnosed in the neonatal period. Congenital diaphragmatic de-fect, also known as Bochdalek hernia, usually occurs with the persistence of the pleuroperitoneal canal in the left posterolateral region of the diaphragm in the embryological period. Although it is rarely seen in the adults, conditions such as intestinal volvulus, strangulation, or perforation with congenital diaphragm defect progress with high mortality and morbidity. In this study, we reported our case that we operated for intrathoracic gastric perforation with congenital diaphragmatic defect. When the patient admitted to the hospital, he had an atypical abdominal pain, significant back pain, and suspicious respiratory complaints. Radiological imaging showed that the stomach and the spleen were located in the left hemithorax due to diaphragmatic hernia also stomach was very dilated. Tachycardia, hypotension, and low saturation developed on the 2nd day of the patient's hospitalization. In the control imaging of the patient, in the left hemithorax, stomach was collapsed and the surrounding appearance compatible with hydropneumothorax, after that findings emergency laparotomy was decided. During the operation, as demonstrated by the radiological findings, a diaphragm defect was seen in the left posterolateral region of the diaphragm. The stomach and spleen were herniated to the left hemithorax from this defect. The stomach and spleen were reduced into the abdomen. The left hemithorax was lavaged with 2000 cc isotonic, left tube thoracostomy was applied, and the diaphragm was repaired. The anterior stomach was primarily repaired. In post-operative follow-up, there were no complications other than wound infection and thoracic tube of the patient was removed. The patient who tolerated enteral food was discharged from hospital with full recovery.
期刊介绍:
The Turkish Journal of Trauma and Emergency Surgery (TJTES) is an official publication of the Turkish Association of Trauma and Emergency Surgery. It is a double-blind and peer-reviewed periodical that considers for publication clinical and experimental studies, case reports, technical contributions, and letters to the editor. Scope of the journal covers the trauma and emergency surgery.
Each submission will be reviewed by at least two external, independent peer reviewers who are experts in their fields in order to ensure an unbiased evaluation process. The editorial board will invite an external and independent reviewer to manage the evaluation processes of manuscripts submitted by editors or by the editorial board members of the journal. The Editor in Chief is the final authority in the decision-making process for all submissions.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
