Weihua Zhang, Jian Zhang, Gaoming Huang, Kaichuang Yang
{"title":"基于积极策略的血肿清除与保守治疗在中度基底神经节出血的管理:一项回顾性研究。","authors":"Weihua Zhang, Jian Zhang, Gaoming Huang, Kaichuang Yang","doi":"10.1515/tnsci-2022-0292","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The internal capsule of the basal ganglia is vulnerable to direct pressure from the hematoma and to secondary damage from toxic products of hemorrhage. Our study evaluated the risk and benefits of active strategies including ultra-early surgery and hematoma evacuation through a transsylvian-transinsular approach for moderate basal ganglia hemorrhage.</p><p><strong>Methods: </strong>We retrospectively collected patients with moderate basal ganglia hemorrhage in two hospitals. The conservative group contained 51 patients who had the best medical treatment, and the surgery group contained 36 patients who were treated with hematoma evacuation through a transsylvian-transinsular approach within 6 h from ictus. Motor function of upper and lower limbs recorded with the motor sub-score of NIHSS (m-NIHSS) at the baseline, 7 days, 30 days, and 90 days, the modified Rankin Scale (mRS), and Barthel Index (BI) scores at 30 and 90 days were compared between the two groups. Good recovery was defined as an m-NIHSS of 0-2 and poor recovery as 3-4. Favorable prognosis was defined as an mRS of 0-3 and unfavorable prognosis as 4-5.</p><p><strong>Results: </strong>The mean time from ictus to surgery was 250.3 ± 57.3 min. The good recovery proportions of upper and lower limbs in the surgery group were significantly higher than that in the conservative group (<i>p</i> < 0.05) at 7 days after hemorrhage. The good recovery proportion of upper limbs was significantly higher in the surgery group than in the conservative group (<i>p</i> < 0.05) at 3 months after hemorrhage. Living ability using BI scores was significantly higher in the surgery group than the conservative group (<i>p</i> < 0.05) at 3 months after hemorrhage. The favorable prognosis proportion had no statistically significant difference between the two groups at 3 months after hemorrhage.</p><p><strong>Conclusions: </strong>Ultra-early hematoma evacuation through a transsylvian-transinsular approach are active strategies for moderate basal ganglia hemorrhage and have potential advantages in improving motor function recovery and daily living. The postoperative rebleeding rate does not increase simultaneously.</p>","PeriodicalId":23227,"journal":{"name":"Translational Neuroscience","volume":"14 1","pages":"20220292"},"PeriodicalIF":2.2000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10388134/pdf/","citationCount":"0","resultStr":"{\"title\":\"Hematoma evacuation based on active strategies versus conservative treatment in the management of moderate basal ganglia hemorrhage: A retrospective study.\",\"authors\":\"Weihua Zhang, Jian Zhang, Gaoming Huang, Kaichuang Yang\",\"doi\":\"10.1515/tnsci-2022-0292\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The internal capsule of the basal ganglia is vulnerable to direct pressure from the hematoma and to secondary damage from toxic products of hemorrhage. Our study evaluated the risk and benefits of active strategies including ultra-early surgery and hematoma evacuation through a transsylvian-transinsular approach for moderate basal ganglia hemorrhage.</p><p><strong>Methods: </strong>We retrospectively collected patients with moderate basal ganglia hemorrhage in two hospitals. The conservative group contained 51 patients who had the best medical treatment, and the surgery group contained 36 patients who were treated with hematoma evacuation through a transsylvian-transinsular approach within 6 h from ictus. Motor function of upper and lower limbs recorded with the motor sub-score of NIHSS (m-NIHSS) at the baseline, 7 days, 30 days, and 90 days, the modified Rankin Scale (mRS), and Barthel Index (BI) scores at 30 and 90 days were compared between the two groups. Good recovery was defined as an m-NIHSS of 0-2 and poor recovery as 3-4. Favorable prognosis was defined as an mRS of 0-3 and unfavorable prognosis as 4-5.</p><p><strong>Results: </strong>The mean time from ictus to surgery was 250.3 ± 57.3 min. The good recovery proportions of upper and lower limbs in the surgery group were significantly higher than that in the conservative group (<i>p</i> < 0.05) at 7 days after hemorrhage. The good recovery proportion of upper limbs was significantly higher in the surgery group than in the conservative group (<i>p</i> < 0.05) at 3 months after hemorrhage. Living ability using BI scores was significantly higher in the surgery group than the conservative group (<i>p</i> < 0.05) at 3 months after hemorrhage. The favorable prognosis proportion had no statistically significant difference between the two groups at 3 months after hemorrhage.</p><p><strong>Conclusions: </strong>Ultra-early hematoma evacuation through a transsylvian-transinsular approach are active strategies for moderate basal ganglia hemorrhage and have potential advantages in improving motor function recovery and daily living. The postoperative rebleeding rate does not increase simultaneously.</p>\",\"PeriodicalId\":23227,\"journal\":{\"name\":\"Translational Neuroscience\",\"volume\":\"14 1\",\"pages\":\"20220292\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10388134/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Translational Neuroscience\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1515/tnsci-2022-0292\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"NEUROSCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational Neuroscience","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1515/tnsci-2022-0292","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"NEUROSCIENCES","Score":null,"Total":0}
Hematoma evacuation based on active strategies versus conservative treatment in the management of moderate basal ganglia hemorrhage: A retrospective study.
Objective: The internal capsule of the basal ganglia is vulnerable to direct pressure from the hematoma and to secondary damage from toxic products of hemorrhage. Our study evaluated the risk and benefits of active strategies including ultra-early surgery and hematoma evacuation through a transsylvian-transinsular approach for moderate basal ganglia hemorrhage.
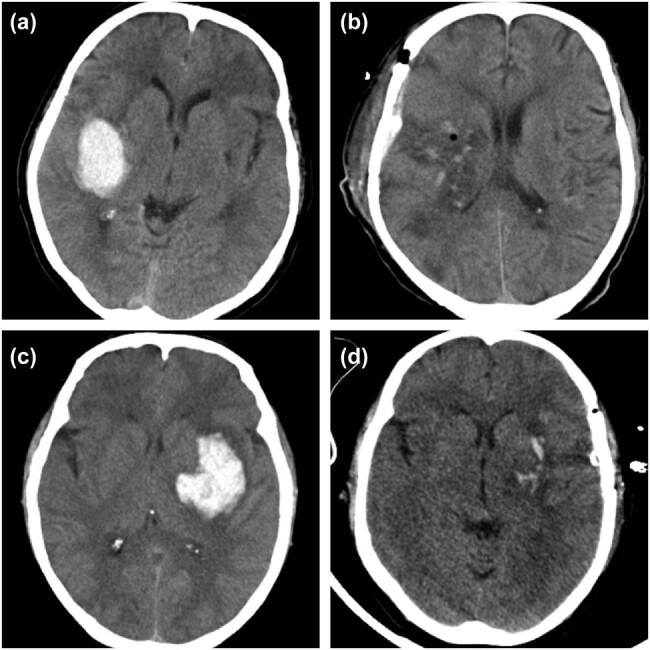
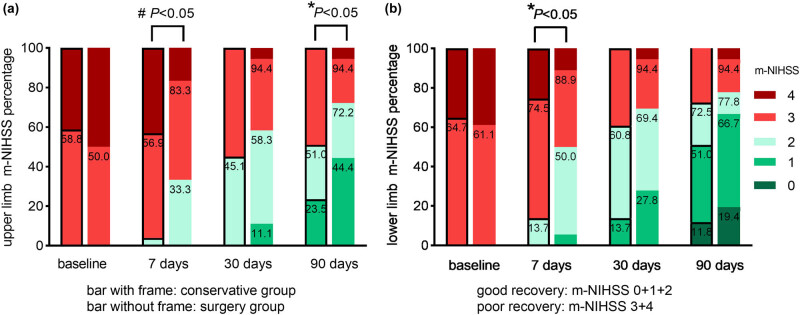
Methods: We retrospectively collected patients with moderate basal ganglia hemorrhage in two hospitals. The conservative group contained 51 patients who had the best medical treatment, and the surgery group contained 36 patients who were treated with hematoma evacuation through a transsylvian-transinsular approach within 6 h from ictus. Motor function of upper and lower limbs recorded with the motor sub-score of NIHSS (m-NIHSS) at the baseline, 7 days, 30 days, and 90 days, the modified Rankin Scale (mRS), and Barthel Index (BI) scores at 30 and 90 days were compared between the two groups. Good recovery was defined as an m-NIHSS of 0-2 and poor recovery as 3-4. Favorable prognosis was defined as an mRS of 0-3 and unfavorable prognosis as 4-5.
Results: The mean time from ictus to surgery was 250.3 ± 57.3 min. The good recovery proportions of upper and lower limbs in the surgery group were significantly higher than that in the conservative group (p < 0.05) at 7 days after hemorrhage. The good recovery proportion of upper limbs was significantly higher in the surgery group than in the conservative group (p < 0.05) at 3 months after hemorrhage. Living ability using BI scores was significantly higher in the surgery group than the conservative group (p < 0.05) at 3 months after hemorrhage. The favorable prognosis proportion had no statistically significant difference between the two groups at 3 months after hemorrhage.
Conclusions: Ultra-early hematoma evacuation through a transsylvian-transinsular approach are active strategies for moderate basal ganglia hemorrhage and have potential advantages in improving motor function recovery and daily living. The postoperative rebleeding rate does not increase simultaneously.
期刊介绍:
Translational Neuroscience provides a closer interaction between basic and clinical neuroscientists to expand understanding of brain structure, function and disease, and translate this knowledge into clinical applications and novel therapies of nervous system disorders.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
