Jason Philip Appleton, Lisa J Woodhouse, Craig S Anderson, Sandeep Ankolekar, Lesley Cala, Mark Dixon, Timothy J England, Kailash Krishnan, Grant Mair, Keith W Muir, John Potter, Christopher I Price, Marc Randall, Thompson G Robinson, Christine Roffe, Else C Sandset, Jeffrey L Saver, Angela Shone, Aloysius Niroshan Siriwardena, Joanna M Wardlaw, Nikola Sprigg, Philip M Bath
{"title":"治疗超急性缺血性中风的院前透皮三硝酸甘油酯:RIGHT-2 随机假对照救护车试验数据。","authors":"Jason Philip Appleton, Lisa J Woodhouse, Craig S Anderson, Sandeep Ankolekar, Lesley Cala, Mark Dixon, Timothy J England, Kailash Krishnan, Grant Mair, Keith W Muir, John Potter, Christopher I Price, Marc Randall, Thompson G Robinson, Christine Roffe, Else C Sandset, Jeffrey L Saver, Angela Shone, Aloysius Niroshan Siriwardena, Joanna M Wardlaw, Nikola Sprigg, Philip M Bath","doi":"10.1136/svn-2022-001634","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The effect of transdermal glyceryl trinitrate (GTN, a nitrovasodilator) on clinical outcome when administered before hospital admission in suspected stroke patients is unclear. Here, we assess the safety and efficacy of GTN in the prespecified subgroup of patients who had an ischaemic stroke within the Rapid Intervention with Glyceryl trinitrate in Hypertensive stroke Trial-2 (RIGHT-2).</p><p><strong>Methods: </strong>RIGHT-2 was an ambulance-based multicentre sham-controlled blinded-endpoint study with patients randomised within 4 hours of onset. The primary outcome was a shift in scores on the modified Rankin scale (mRS) at day 90. Secondary outcomes included death; a global analysis (Wei-Lachin test) containing Barthel Index, EuroQol-5D, mRS, telephone interview for cognitive status-modified and Zung depression scale; and neuroimaging-determined 'brain frailty' markers. Data were reported as n (%), mean (SD), median [IQR], adjusted common OR (acOR), mean difference or Mann-Whitney difference (MWD) with 95% CI.</p><p><strong>Results: </strong>597 of 1149 (52%) patients had a final diagnosis of ischaemic stroke; age 75 (12) years, premorbid mRS>2 107 (18%), Glasgow Coma Scale 14 (2) and time from onset to randomisation 67 [45, 108] min. Neuroimaging 'brain frailty' was common: median score 2 [2, 3] (range 0-3). At day 90, GTN did not influence the primary outcome (acOR for increased disability 1.15, 95% CI 0.85 to 1.54), death or global analysis (MWD 0.00, 95% CI -0.10 to 0.09). In subgroup analyses, there were non-significant interactions suggesting GTN may be associated with more death and dependency in participants randomised within 1 hour of symptom onset and in those with more severe stroke.</p><p><strong>Conclusions: </strong>In patients who had an ischaemic stroke, ultra-acute administration of transdermal GTN in the ambulance did not improve clinical outcomes in a population with more clinical and radiological frailty than seen in previous in-hospital trials.</p>","PeriodicalId":22021,"journal":{"name":"Stroke and Vascular Neurology","volume":" ","pages":"38-49"},"PeriodicalIF":4.9000,"publicationDate":"2024-02-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10956104/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prehospital transdermal glyceryl trinitrate for ultra-acute ischaemic stroke: data from the RIGHT-2 randomised sham-controlled ambulance trial.\",\"authors\":\"Jason Philip Appleton, Lisa J Woodhouse, Craig S Anderson, Sandeep Ankolekar, Lesley Cala, Mark Dixon, Timothy J England, Kailash Krishnan, Grant Mair, Keith W Muir, John Potter, Christopher I Price, Marc Randall, Thompson G Robinson, Christine Roffe, Else C Sandset, Jeffrey L Saver, Angela Shone, Aloysius Niroshan Siriwardena, Joanna M Wardlaw, Nikola Sprigg, Philip M Bath\",\"doi\":\"10.1136/svn-2022-001634\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The effect of transdermal glyceryl trinitrate (GTN, a nitrovasodilator) on clinical outcome when administered before hospital admission in suspected stroke patients is unclear. Here, we assess the safety and efficacy of GTN in the prespecified subgroup of patients who had an ischaemic stroke within the Rapid Intervention with Glyceryl trinitrate in Hypertensive stroke Trial-2 (RIGHT-2).</p><p><strong>Methods: </strong>RIGHT-2 was an ambulance-based multicentre sham-controlled blinded-endpoint study with patients randomised within 4 hours of onset. The primary outcome was a shift in scores on the modified Rankin scale (mRS) at day 90. Secondary outcomes included death; a global analysis (Wei-Lachin test) containing Barthel Index, EuroQol-5D, mRS, telephone interview for cognitive status-modified and Zung depression scale; and neuroimaging-determined 'brain frailty' markers. Data were reported as n (%), mean (SD), median [IQR], adjusted common OR (acOR), mean difference or Mann-Whitney difference (MWD) with 95% CI.</p><p><strong>Results: </strong>597 of 1149 (52%) patients had a final diagnosis of ischaemic stroke; age 75 (12) years, premorbid mRS>2 107 (18%), Glasgow Coma Scale 14 (2) and time from onset to randomisation 67 [45, 108] min. Neuroimaging 'brain frailty' was common: median score 2 [2, 3] (range 0-3). At day 90, GTN did not influence the primary outcome (acOR for increased disability 1.15, 95% CI 0.85 to 1.54), death or global analysis (MWD 0.00, 95% CI -0.10 to 0.09). In subgroup analyses, there were non-significant interactions suggesting GTN may be associated with more death and dependency in participants randomised within 1 hour of symptom onset and in those with more severe stroke.</p><p><strong>Conclusions: </strong>In patients who had an ischaemic stroke, ultra-acute administration of transdermal GTN in the ambulance did not improve clinical outcomes in a population with more clinical and radiological frailty than seen in previous in-hospital trials.</p>\",\"PeriodicalId\":22021,\"journal\":{\"name\":\"Stroke and Vascular Neurology\",\"volume\":\" \",\"pages\":\"38-49\"},\"PeriodicalIF\":4.9000,\"publicationDate\":\"2024-02-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10956104/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Stroke and Vascular Neurology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/svn-2022-001634\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke and Vascular Neurology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/svn-2022-001634","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:疑似脑卒中患者入院前使用透皮三硝酸甘油酯(GTN,一种硝基血管扩张剂)对临床预后的影响尚不明确。在此,我们评估了 GTN 在高血压脑卒中三硝酸甘油快速干预试验-2(RIGHT-2)的缺血性脑卒中患者预设亚组中的安全性和有效性:RIGHT-2是一项基于救护车的多中心假对照盲法终点研究,患者在发病4小时内被随机分组。主要结果是第90天时改良Rankin量表(mRS)评分的变化。次要结果包括死亡;包含Barthel指数、EuroQol-5D、mRS、改良认知状态电话访谈和Zung抑郁量表的总体分析(Wei-Lachin测试);以及神经影像学确定的 "大脑虚弱 "标志物。数据以 n (%)、平均值 (SD)、中位数 [IQR]、调整后的普通 OR (acOR)、平均差或带有 95% CI 的 Mann-Whitney 差异 (MWD) 表示:1149名患者中有597名(52%)最终诊断为缺血性卒中;年龄75(12)岁,病前mRS>2 107(18%),格拉斯哥昏迷量表14(2),发病至随机化时间67 [45, 108]分钟。神经影像学 "脑衰弱 "很常见:中位数为 2 [2, 3](范围 0-3)。在第 90 天,GTN 不会影响主要结果(残疾增加的 acOR 为 1.15,95% CI 为 0.85 至 1.54)、死亡或总体分析(MWD 为 0.00,95% CI 为 -0.10 至 0.09)。在亚组分析中,存在不显著的交互作用,表明在症状出现后1小时内随机接受治疗的参与者以及中风程度更严重的患者中,GTN可能与更多的死亡和依赖性相关:对于缺血性脑卒中患者,与以往的院内试验相比,在临床和影像学上更虚弱的人群中,在救护车上超短时间内给予经皮GTN并不能改善临床预后。
Prehospital transdermal glyceryl trinitrate for ultra-acute ischaemic stroke: data from the RIGHT-2 randomised sham-controlled ambulance trial.
Background: The effect of transdermal glyceryl trinitrate (GTN, a nitrovasodilator) on clinical outcome when administered before hospital admission in suspected stroke patients is unclear. Here, we assess the safety and efficacy of GTN in the prespecified subgroup of patients who had an ischaemic stroke within the Rapid Intervention with Glyceryl trinitrate in Hypertensive stroke Trial-2 (RIGHT-2).
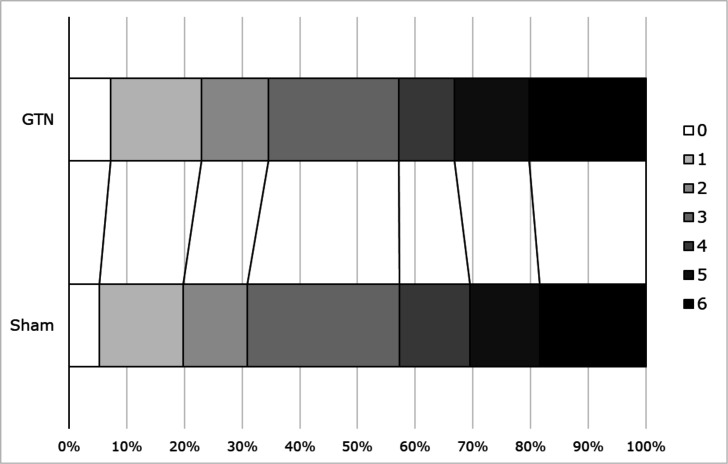
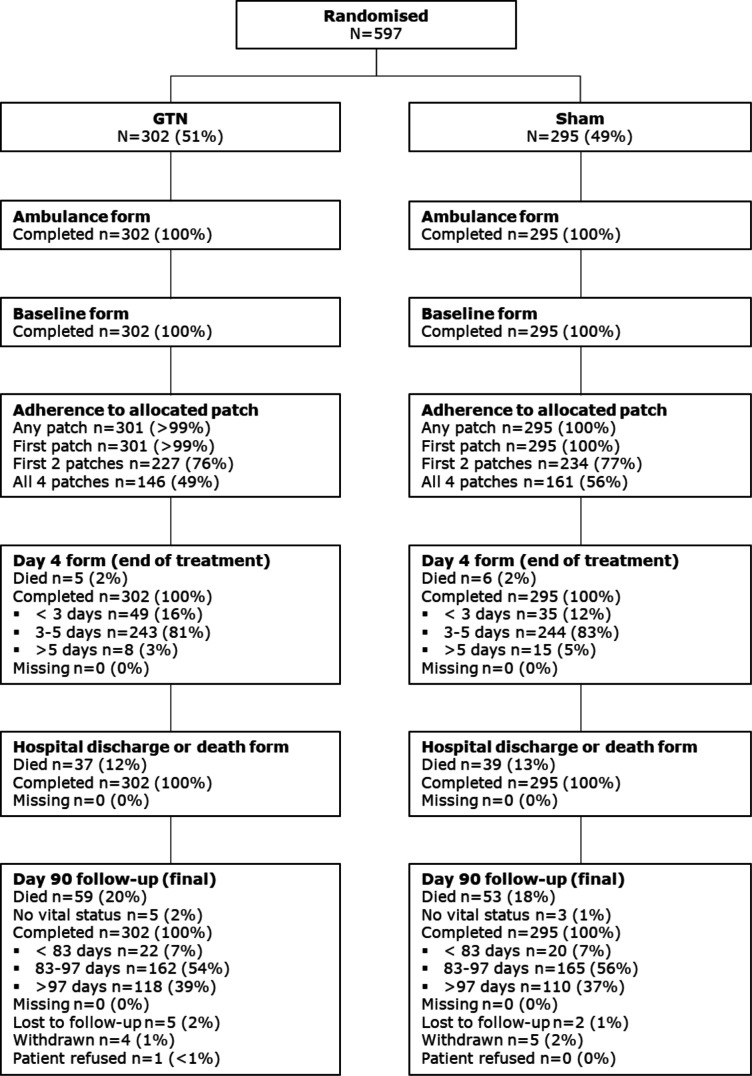
Methods: RIGHT-2 was an ambulance-based multicentre sham-controlled blinded-endpoint study with patients randomised within 4 hours of onset. The primary outcome was a shift in scores on the modified Rankin scale (mRS) at day 90. Secondary outcomes included death; a global analysis (Wei-Lachin test) containing Barthel Index, EuroQol-5D, mRS, telephone interview for cognitive status-modified and Zung depression scale; and neuroimaging-determined 'brain frailty' markers. Data were reported as n (%), mean (SD), median [IQR], adjusted common OR (acOR), mean difference or Mann-Whitney difference (MWD) with 95% CI.
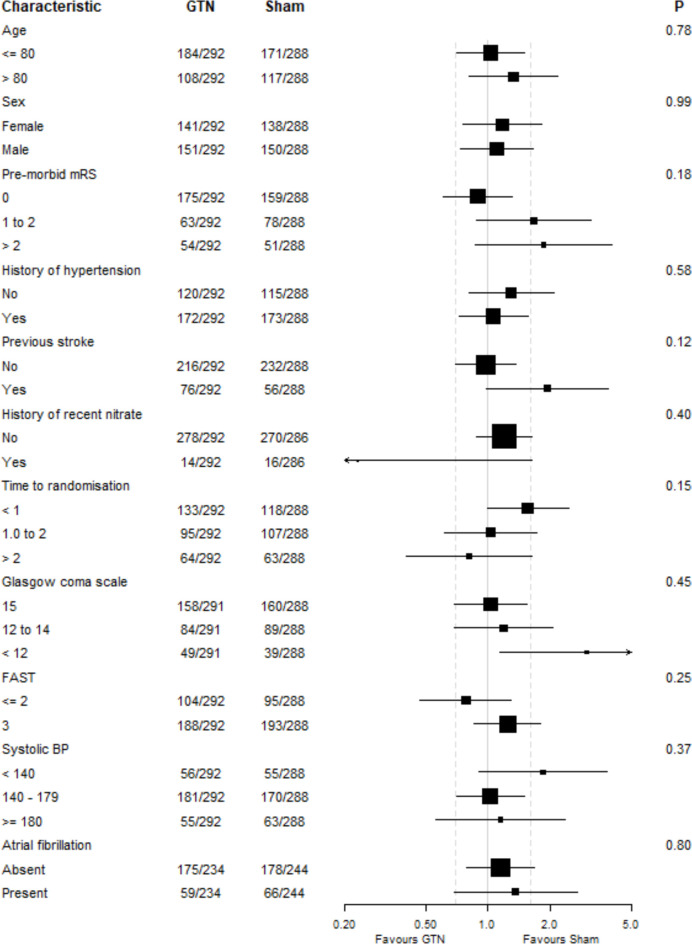
Results: 597 of 1149 (52%) patients had a final diagnosis of ischaemic stroke; age 75 (12) years, premorbid mRS>2 107 (18%), Glasgow Coma Scale 14 (2) and time from onset to randomisation 67 [45, 108] min. Neuroimaging 'brain frailty' was common: median score 2 [2, 3] (range 0-3). At day 90, GTN did not influence the primary outcome (acOR for increased disability 1.15, 95% CI 0.85 to 1.54), death or global analysis (MWD 0.00, 95% CI -0.10 to 0.09). In subgroup analyses, there were non-significant interactions suggesting GTN may be associated with more death and dependency in participants randomised within 1 hour of symptom onset and in those with more severe stroke.
Conclusions: In patients who had an ischaemic stroke, ultra-acute administration of transdermal GTN in the ambulance did not improve clinical outcomes in a population with more clinical and radiological frailty than seen in previous in-hospital trials.
期刊介绍:
Stroke and Vascular Neurology (SVN) is the official journal of the Chinese Stroke Association. Supported by a team of renowned Editors, and fully Open Access, the journal encourages debate on controversial techniques, issues on health policy and social medicine.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
