James Mannion, Kathryn Hong, Sarah-Jane Lennon, Anthony Kenny, Joseph Galvin, Jim O'Brien, Gael Jauvert, Edward Keelan, Usama Boles
{"title":"用新型自动电压分析比较窦性心律和心房颤动的左心房低压区:一项初步研究。","authors":"James Mannion, Kathryn Hong, Sarah-Jane Lennon, Anthony Kenny, Joseph Galvin, Jim O'Brien, Gael Jauvert, Edward Keelan, Usama Boles","doi":"10.14740/cr1503","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Low voltage areas (LVAs) have been proposed as surrogate markers for left atrial (LA) scar. Correlation between voltages in sinus rhythm (SR) and atrial fibrillation (AF) have previously been measured via point-by-point analysis. We sought to compare LA voltage composition measured in SR to AF, utilizing a high-density automated voltage histogram analysis (VHA) tool in those undergoing pulmonary vein isolation (PVI) for persistent AF (PeAF).</p><p><strong>Methods: </strong>We retrospectively analyzed patients with PeAF undergoing <i>de novo</i> PVI. Maps required ≥ 1,000 voltage points in each rhythm and had a standardized procedure (mapped in AF then remapped in SR post-PVI). We created six anatomical segments (AS) from each map: anterior, posterior, roof, floor, septal and lateral AS. These were analyzed by VHA, categorizing atrial LVAs into 10 voltage aliquots 0 - 0.5 mV. Data were analyzed using SPSS v.26.</p><p><strong>Results: </strong>We acquired 58,342 voltage points (n = 10 patients, mean age: 67 ± 13 years, three females). LVA burdens of ≤ 0.2 mV, designated as \"severe LVAs\", were comparable between most AS (except on the posterior wall) with good correlation. Mapped voltages between the ranges of 0.21 and 0.5 mV were labeled as \"diseased LA tissue\", and these were found significantly more in AF than SR. Significant differences were seen on the roof, anterior, posterior, and lateral AS.</p><p><strong>Conclusions: </strong>Diseased LA tissue (0.21 - 0.5 mV) burden is significantly higher in AF than SR, mainly in the anterior, roof, lateral, and posterior wall. LA \"severe LVA\" (≤ 0.2 mV) burden is comparable in both rhythms, except with respect to the posterior wall. Our findings suggest that mapping rhythm has less effect on the LA with voltages < 0.2 mV than 0.2 - 0.5 mV across all anatomical regions, excluding the posterior wall.</p>","PeriodicalId":9424,"journal":{"name":"Cardiology Research","volume":"14 4","pages":"268-278"},"PeriodicalIF":1.4000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1f/ab/cr-14-268.PMC10409550.pdf","citationCount":"0","resultStr":"{\"title\":\"Comparing Left Atrial Low Voltage Areas in Sinus Rhythm and Atrial Fibrillation Using Novel Automated Voltage Analysis: A Pilot Study.\",\"authors\":\"James Mannion, Kathryn Hong, Sarah-Jane Lennon, Anthony Kenny, Joseph Galvin, Jim O'Brien, Gael Jauvert, Edward Keelan, Usama Boles\",\"doi\":\"10.14740/cr1503\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Low voltage areas (LVAs) have been proposed as surrogate markers for left atrial (LA) scar. Correlation between voltages in sinus rhythm (SR) and atrial fibrillation (AF) have previously been measured via point-by-point analysis. We sought to compare LA voltage composition measured in SR to AF, utilizing a high-density automated voltage histogram analysis (VHA) tool in those undergoing pulmonary vein isolation (PVI) for persistent AF (PeAF).</p><p><strong>Methods: </strong>We retrospectively analyzed patients with PeAF undergoing <i>de novo</i> PVI. Maps required ≥ 1,000 voltage points in each rhythm and had a standardized procedure (mapped in AF then remapped in SR post-PVI). We created six anatomical segments (AS) from each map: anterior, posterior, roof, floor, septal and lateral AS. These were analyzed by VHA, categorizing atrial LVAs into 10 voltage aliquots 0 - 0.5 mV. Data were analyzed using SPSS v.26.</p><p><strong>Results: </strong>We acquired 58,342 voltage points (n = 10 patients, mean age: 67 ± 13 years, three females). LVA burdens of ≤ 0.2 mV, designated as \\\"severe LVAs\\\", were comparable between most AS (except on the posterior wall) with good correlation. Mapped voltages between the ranges of 0.21 and 0.5 mV were labeled as \\\"diseased LA tissue\\\", and these were found significantly more in AF than SR. Significant differences were seen on the roof, anterior, posterior, and lateral AS.</p><p><strong>Conclusions: </strong>Diseased LA tissue (0.21 - 0.5 mV) burden is significantly higher in AF than SR, mainly in the anterior, roof, lateral, and posterior wall. LA \\\"severe LVA\\\" (≤ 0.2 mV) burden is comparable in both rhythms, except with respect to the posterior wall. Our findings suggest that mapping rhythm has less effect on the LA with voltages < 0.2 mV than 0.2 - 0.5 mV across all anatomical regions, excluding the posterior wall.</p>\",\"PeriodicalId\":9424,\"journal\":{\"name\":\"Cardiology Research\",\"volume\":\"14 4\",\"pages\":\"268-278\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1f/ab/cr-14-268.PMC10409550.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/cr1503\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/cr1503","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Comparing Left Atrial Low Voltage Areas in Sinus Rhythm and Atrial Fibrillation Using Novel Automated Voltage Analysis: A Pilot Study.
Background: Low voltage areas (LVAs) have been proposed as surrogate markers for left atrial (LA) scar. Correlation between voltages in sinus rhythm (SR) and atrial fibrillation (AF) have previously been measured via point-by-point analysis. We sought to compare LA voltage composition measured in SR to AF, utilizing a high-density automated voltage histogram analysis (VHA) tool in those undergoing pulmonary vein isolation (PVI) for persistent AF (PeAF).
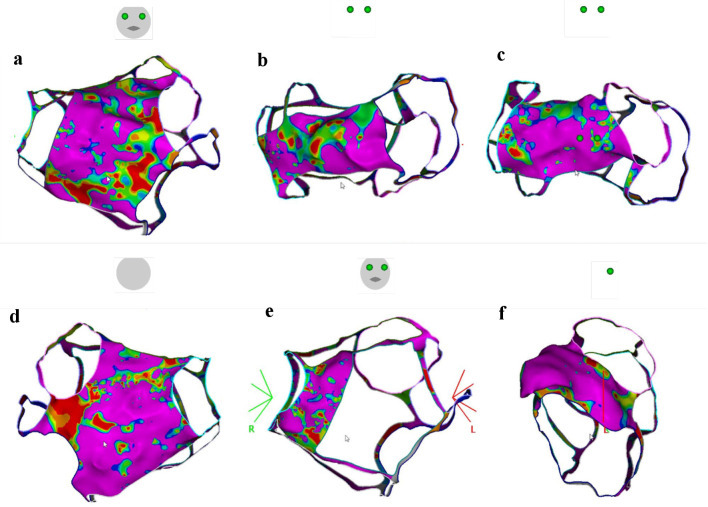
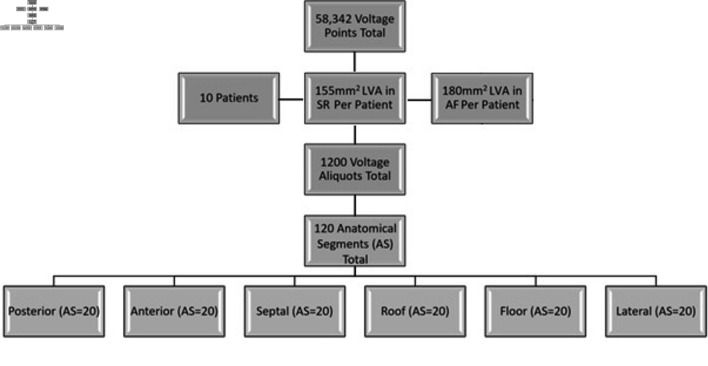
Methods: We retrospectively analyzed patients with PeAF undergoing de novo PVI. Maps required ≥ 1,000 voltage points in each rhythm and had a standardized procedure (mapped in AF then remapped in SR post-PVI). We created six anatomical segments (AS) from each map: anterior, posterior, roof, floor, septal and lateral AS. These were analyzed by VHA, categorizing atrial LVAs into 10 voltage aliquots 0 - 0.5 mV. Data were analyzed using SPSS v.26.
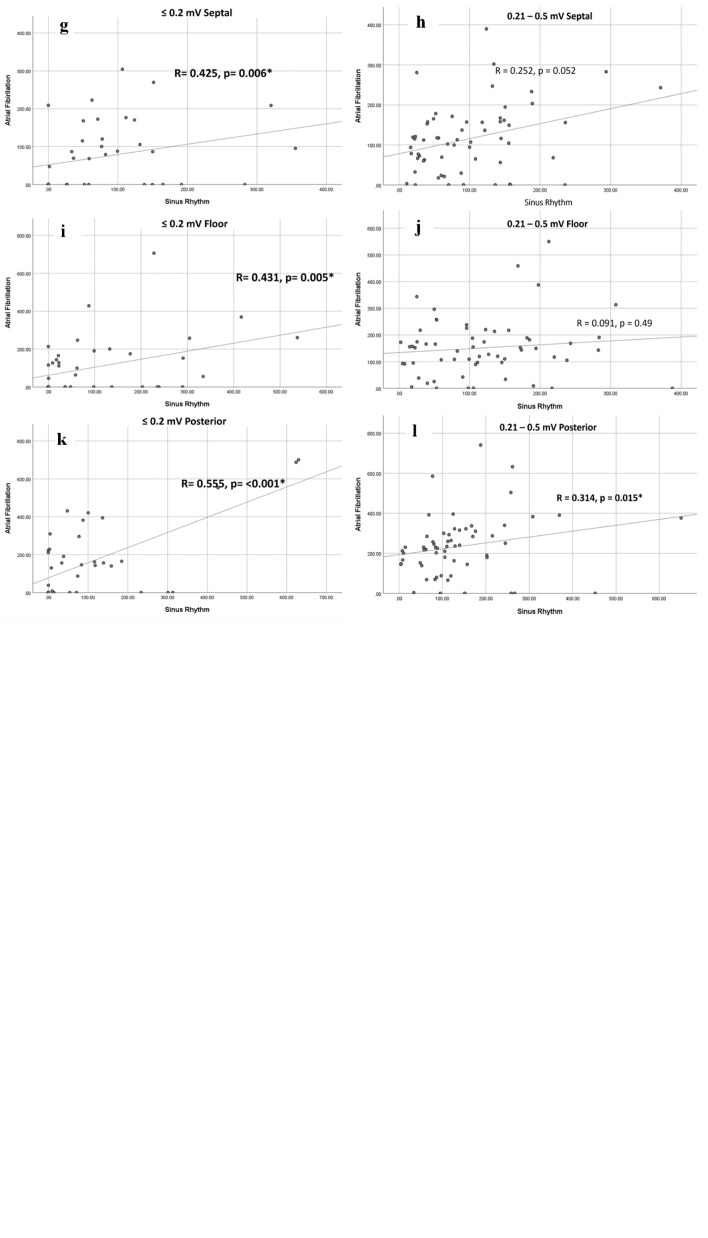
Results: We acquired 58,342 voltage points (n = 10 patients, mean age: 67 ± 13 years, three females). LVA burdens of ≤ 0.2 mV, designated as "severe LVAs", were comparable between most AS (except on the posterior wall) with good correlation. Mapped voltages between the ranges of 0.21 and 0.5 mV were labeled as "diseased LA tissue", and these were found significantly more in AF than SR. Significant differences were seen on the roof, anterior, posterior, and lateral AS.
Conclusions: Diseased LA tissue (0.21 - 0.5 mV) burden is significantly higher in AF than SR, mainly in the anterior, roof, lateral, and posterior wall. LA "severe LVA" (≤ 0.2 mV) burden is comparable in both rhythms, except with respect to the posterior wall. Our findings suggest that mapping rhythm has less effect on the LA with voltages < 0.2 mV than 0.2 - 0.5 mV across all anatomical regions, excluding the posterior wall.
期刊介绍:
Cardiology Research is an open access, peer-reviewed, international journal. All submissions relating to basic research and clinical practice of cardiology and cardiovascular medicine are in this journal''s scope. This journal focuses on publishing original research and observations in all cardiovascular medicine aspects. Manuscript types include original article, review, case report, short communication, book review, letter to the editor.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
