Alberto Palazzuoli MD, PhD, FESC , Alessandra Cartocci PhD , Filippo Pirrotta MD , Francesca Vannuccini MD , Alessandro Campora MD , Luca Martini MD , Frank Loyd Dini MD , Erberto Carluccio MD, FEACVI , Gaetano Ruocco MD
{"title":"Different right ventricular dysfunction and pulmonary coupling in acute heart failure according to the left ventricular ejection fraction","authors":"Alberto Palazzuoli MD, PhD, FESC , Alessandra Cartocci PhD , Filippo Pirrotta MD , Francesca Vannuccini MD , Alessandro Campora MD , Luca Martini MD , Frank Loyd Dini MD , Erberto Carluccio MD, FEACVI , Gaetano Ruocco MD","doi":"10.1016/j.pcad.2023.07.008","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p><span>Right ventricular (RV) dysfunction and pulmonary uncoupling are two acknowledged features associated with poor outcome, however few data defined RV adaptation across the different left ventricular ejection fraction (EF) cut-off. Additionally, less data are reported </span>in patients<span> with acute heart failure (AHF).</span></p></div><div><h3>Aims</h3><p>The aim of present study was to analyse RV function<span> in AHF patients presenting with either reduced or preserved EF.</span></p></div><div><h3>Methods</h3><p>This is a multi-center observational study including 380 patients affected by AHF: 235 had AHF with reduced EF (AHFrEF) and 145 had AHF with preserved EF<span> (AHFpEF). Pulmonary artery systolic pressure<span> (PASP), tricuspid annular plane systolic excursion (TAPSE), S′ wave velocity, and the RV end-diastolic diameter (RVEDD) were measured by echocardiography. TAPSE/PASP and S′/PASP ratios were calculated as non-invasive surrogates of RV-pulmonary arterial coupling.</span></span></p></div><div><h3>Results</h3><p>Factors associated with poor outcome were higher values of PASP (45 [40–55] mmHg vs 40 [35–46] mmHg; <em>p</em> < 0.001), RVEDD (44 [38–47] mm vs 37 [35–42] mm; p < 0.001), lower TAPSE values (17 [15–20] mm vs 20 [18–22] mm; <em>p</em> < 0.001) and S′ wave (10 [8–12] cm/s vs 11 [10–13] cm/s; <em>p</em> < 0.001), reduced TAPSE/PASP (0.37 [0.29–0.47] vs 0.50 [0.40–0.60]; p < 0.001) and S′/PASP ratios (0.22 [0.18–0.28] vs 0.28 [0.22–0.34]; p < 0.001). However, the prognostic parameters differed according to the LVEF value: in AHFpEF S′/PASP between 0.22 and 0.29 and > 0.29 demonstrated a protective prognostic value (Respectively HR 0.29 (0.16–0.53), <em>p</em> < 0.001 and HR 0.22 [0.12–0.42], p < 0.001). Conversely, in AHFrEF, TAPSE <16 mm (HR 2.59 [1.67–4.03], p < 0.001), ICV > 21 mm (HR 1.17 [1.17–1.28], <em>p</em> = 0.001) and TAPSE/PASP <0.49 HR 1.92 [1.10–3.37], <em>p</em><span> = 0.023) were related to adverse outcome.</span></p></div><div><h3>Conclusions</h3><p>RV adaptation and RV pulmonary coupling differ in AHF according to the level of LVEF. S′ wave, and S′/PASP are associated with adverse outcome in patients with preserved EF; reduced TAPSE and TAPSE/PASP are better prognostic predictors in patients with reduced EF.</p></div>","PeriodicalId":21156,"journal":{"name":"Progress in cardiovascular diseases","volume":"81 ","pages":"Pages 89-97"},"PeriodicalIF":7.6000,"publicationDate":"2023-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Progress in cardiovascular diseases","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0033062023000749","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/2 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background
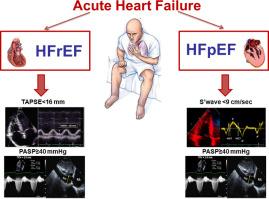
Right ventricular (RV) dysfunction and pulmonary uncoupling are two acknowledged features associated with poor outcome, however few data defined RV adaptation across the different left ventricular ejection fraction (EF) cut-off. Additionally, less data are reported in patients with acute heart failure (AHF).
Aims
The aim of present study was to analyse RV function in AHF patients presenting with either reduced or preserved EF.
Methods
This is a multi-center observational study including 380 patients affected by AHF: 235 had AHF with reduced EF (AHFrEF) and 145 had AHF with preserved EF (AHFpEF). Pulmonary artery systolic pressure (PASP), tricuspid annular plane systolic excursion (TAPSE), S′ wave velocity, and the RV end-diastolic diameter (RVEDD) were measured by echocardiography. TAPSE/PASP and S′/PASP ratios were calculated as non-invasive surrogates of RV-pulmonary arterial coupling.
Results
Factors associated with poor outcome were higher values of PASP (45 [40–55] mmHg vs 40 [35–46] mmHg; p < 0.001), RVEDD (44 [38–47] mm vs 37 [35–42] mm; p < 0.001), lower TAPSE values (17 [15–20] mm vs 20 [18–22] mm; p < 0.001) and S′ wave (10 [8–12] cm/s vs 11 [10–13] cm/s; p < 0.001), reduced TAPSE/PASP (0.37 [0.29–0.47] vs 0.50 [0.40–0.60]; p < 0.001) and S′/PASP ratios (0.22 [0.18–0.28] vs 0.28 [0.22–0.34]; p < 0.001). However, the prognostic parameters differed according to the LVEF value: in AHFpEF S′/PASP between 0.22 and 0.29 and > 0.29 demonstrated a protective prognostic value (Respectively HR 0.29 (0.16–0.53), p < 0.001 and HR 0.22 [0.12–0.42], p < 0.001). Conversely, in AHFrEF, TAPSE <16 mm (HR 2.59 [1.67–4.03], p < 0.001), ICV > 21 mm (HR 1.17 [1.17–1.28], p = 0.001) and TAPSE/PASP <0.49 HR 1.92 [1.10–3.37], p = 0.023) were related to adverse outcome.
Conclusions
RV adaptation and RV pulmonary coupling differ in AHF according to the level of LVEF. S′ wave, and S′/PASP are associated with adverse outcome in patients with preserved EF; reduced TAPSE and TAPSE/PASP are better prognostic predictors in patients with reduced EF.
期刊介绍:
Progress in Cardiovascular Diseases provides comprehensive coverage of a single topic related to heart and circulatory disorders in each issue. Some issues include special articles, definitive reviews that capture the state of the art in the management of particular clinical problems in cardiology.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
