{"title":"Calcified plaque harboring lipidic materials associates with no-reflow phenomenon after PCI in stable CAD.","authors":"Hayato Hosoda, Yu Kataoka, Stephen J Nicholls, Rishi Puri, Kota Murai, Satoshi Kitahara, Kentaro Mitsui, Hiroki Sugane, Kenichiro Sawada, Takamasa Iwai, Hideo Matama, Satoshi Honda, Kensuke Takagi, Masashi Fujino, Shuichi Yoneda, Fumiyuki Otsuka, Itaru Takamisawa, Kensaku Nishihira, Yasuhide Asaumi, Kazuya Kawai, Teruo Noguchi","doi":"10.1007/s10554-023-02905-y","DOIUrl":null,"url":null,"abstract":"<p><p>Calcified atheroma has been viewed conventionally as stable lesion which less likely increases no-reflow phenomenon. Given that lipidic materials triggers the formation of calcification, lipidic materials could exist within calcified lesion, which may cause no-reflow phenomenon after PCI. The REASSURE-NIRS registry (NCT04864171) employed near-infrared spectroscopy and intravascular ultrasound imaging to evaluate maximum 4-mm lipid-core burden index (maxLCBI<sub>4mm</sub>) at target lesions containing small (maximum calcification arc < 180°: n = 272) and large calcification (maximum calcification arc ≥ 180°: n = 189) in stable CAD patients. The associations of maxLCBI<sub>4mm</sub> with corrected TIMI frame count (CTFC) and no-reflow phenomenon after PCI were analyzed in patients with target lesions containing small and large calcification, respectively. No-reflow phenomenon occurred in 8.0% of study population. Receiver-operating characteristics curve analyses revealed that optimal cut-off values of maxLCBI<sub>4mm</sub> for predicting no-reflow phenomenon were 585 at small calcification (AUC = 0.72, p < 0.001) and 679 at large calcification (AUC = 0.76, p = 0.001). Target lesions containing small calcification with maxLCBI<sub>4mm</sub> ≥ 585 more likely exhibited a greater CTFC (p < 0.001). In those with large calcification, 55.6% of them had maxLCBI<sub>4mm</sub> ≥ 400 [vs. 56.2% (small calcification), p = 0.82]. Furthermore, a higher CTFC (p < 0.001) was observed in association with maxLCBI<sub>4mm</sub> ≥ 679 at large calcification. On multivariable analysis, maxLCBI<sub>4mm</sub> at large calcification still independently predicted no-reflow phenomenon (OR = 1.60, 95%CI = 1.32-1.94, p < 0.001). MaxLCBI<sub>4mm</sub> at target lesions exhibiting large calcification elevated a risk of no-reflow phenomenon after PCI. Calcified plaque containing lipidic materials is not necessarily stable lesion, but could be active and high-risk one causing no-reflow phenomenon.</p>","PeriodicalId":50332,"journal":{"name":"International Journal of Cardiovascular Imaging","volume":" ","pages":"1927-1941"},"PeriodicalIF":1.5000,"publicationDate":"2023-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10589149/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Cardiovascular Imaging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10554-023-02905-y","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
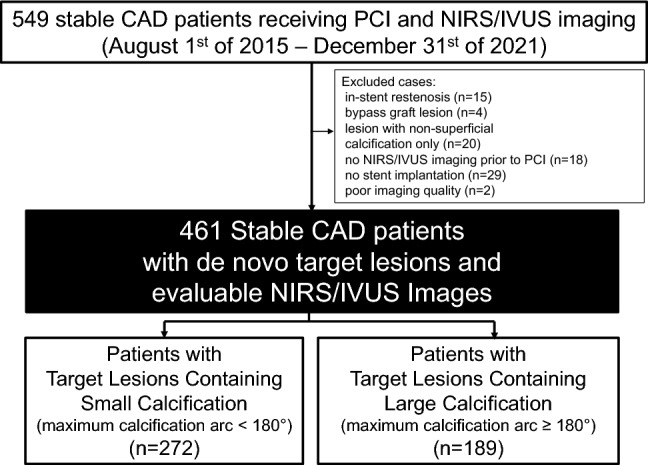
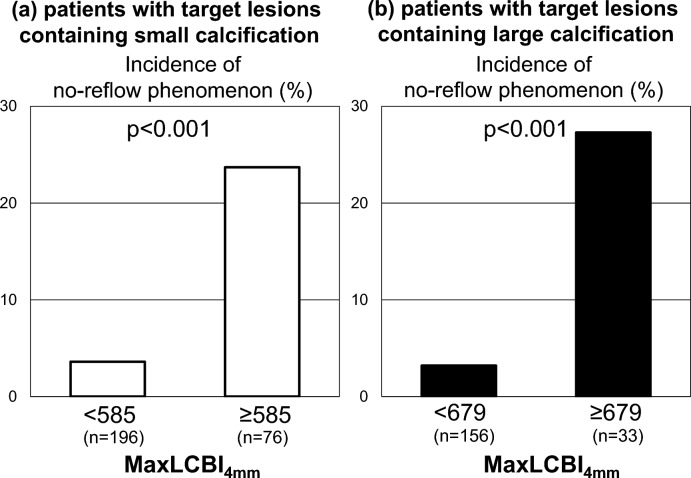
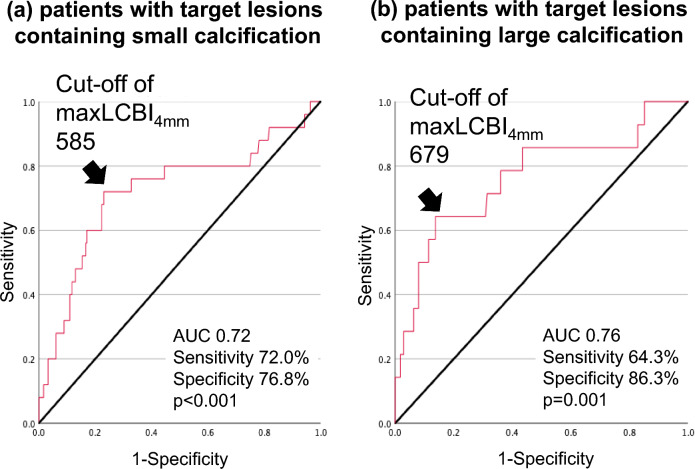
Calcified atheroma has been viewed conventionally as stable lesion which less likely increases no-reflow phenomenon. Given that lipidic materials triggers the formation of calcification, lipidic materials could exist within calcified lesion, which may cause no-reflow phenomenon after PCI. The REASSURE-NIRS registry (NCT04864171) employed near-infrared spectroscopy and intravascular ultrasound imaging to evaluate maximum 4-mm lipid-core burden index (maxLCBI4mm) at target lesions containing small (maximum calcification arc < 180°: n = 272) and large calcification (maximum calcification arc ≥ 180°: n = 189) in stable CAD patients. The associations of maxLCBI4mm with corrected TIMI frame count (CTFC) and no-reflow phenomenon after PCI were analyzed in patients with target lesions containing small and large calcification, respectively. No-reflow phenomenon occurred in 8.0% of study population. Receiver-operating characteristics curve analyses revealed that optimal cut-off values of maxLCBI4mm for predicting no-reflow phenomenon were 585 at small calcification (AUC = 0.72, p < 0.001) and 679 at large calcification (AUC = 0.76, p = 0.001). Target lesions containing small calcification with maxLCBI4mm ≥ 585 more likely exhibited a greater CTFC (p < 0.001). In those with large calcification, 55.6% of them had maxLCBI4mm ≥ 400 [vs. 56.2% (small calcification), p = 0.82]. Furthermore, a higher CTFC (p < 0.001) was observed in association with maxLCBI4mm ≥ 679 at large calcification. On multivariable analysis, maxLCBI4mm at large calcification still independently predicted no-reflow phenomenon (OR = 1.60, 95%CI = 1.32-1.94, p < 0.001). MaxLCBI4mm at target lesions exhibiting large calcification elevated a risk of no-reflow phenomenon after PCI. Calcified plaque containing lipidic materials is not necessarily stable lesion, but could be active and high-risk one causing no-reflow phenomenon.
期刊介绍:
The International Journal of Cardiovascular Imaging publishes technical and clinical communications (original articles, review articles and editorial comments) associated with cardiovascular diseases. The technical communications include the research, development and evaluation of novel imaging methods in the various imaging domains. These domains include magnetic resonance imaging, computed tomography, X-ray imaging, intravascular imaging, and applications in nuclear cardiology and echocardiography, and any combination of these techniques. Of particular interest are topics in medical image processing and image-guided interventions. Clinical applications of such imaging techniques include improved diagnostic approaches, treatment , prognosis and follow-up of cardiovascular patients. Topics include: multi-center or larger individual studies dealing with risk stratification and imaging utilization, applications for better characterization of cardiovascular diseases, and assessment of the efficacy of new drugs and interventional devices.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
