Adam R Schertz, Ashley E Eisner, Sydney A Smith, Kristin M Lenoir, Karl W Thomas
{"title":"Clinical Phenotypes of Sepsis in a Cohort of Hospitalized Patients According to Infection Site.","authors":"Adam R Schertz, Ashley E Eisner, Sydney A Smith, Kristin M Lenoir, Karl W Thomas","doi":"10.1097/CCE.0000000000000955","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Clinical sepsis phenotypes may be defined by a wide range of characteristics such as site of infection, organ dysfunction patterns, laboratory values, and demographics. There is a paucity of literature regarding the impact of site of infection on the timing and pattern of clinical sepsis markers. This study hypothesizes that important phenotypic variation in clinical markers and outcomes of sepsis exists when stratified by infection site.</p><p><strong>Design: </strong>Retrospective cohort study.</p><p><strong>Setting: </strong>Five hospitals within the Wake Forest Health System from June 2019 to December 2019.</p><p><strong>Patients: </strong>Six thousand seven hundred fifty-three hospitalized adults with a discharge <i>International Classification of Diseases</i>, 10th Revision code for acute infection who met systemic inflammatory response syndrome (SIRS), quick Sepsis-related Organ Failure Assessment (qSOFA), or Sequential Organ Failure Assessment (SOFA) criteria during the index hospitalization.</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>The primary outcome of interest was a composite of 30-day mortality or shock. Infection site was determined by a two-reviewer process. Significant demographic, vital sign, and laboratory result differences were seen across all infection sites. For the composite outcome of shock or 30-day mortality, unknown or unspecified infections had the highest proportion (21.34%) and CNS infections had the lowest proportion (8.11%). Respiratory, vascular, and unknown or unspecified infection sites showed a significantly increased adjusted and unadjusted odds of the composite outcome as compared with the other infection sites except CNS. Hospital time prior to SIRS positivity was shortest in unknown or unspecified infections at a median of 0.88 hours (interquartile range [IQR], 0.22-5.05 hr), and hospital time prior to qSOFA and SOFA positivity was shortest in respiratory infections at a median of 54.83 hours (IQR, 9.55-104.67 hr) and 1.88 hours (IQR, 0.47-17.40 hr), respectively.</p><p><strong>Conclusions: </strong>Phenotypic variation in illness severity and mortality exists when stratified by infection site. There is a significantly higher adjusted and unadjusted odds of the composite outcome of 30-day mortality or shock in respiratory, vascular, and unknown or unspecified infections as compared with other sites.</p>","PeriodicalId":10759,"journal":{"name":"Critical Care Explorations","volume":"5 8","pages":"e0955"},"PeriodicalIF":0.0000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/7a/18/cc9-5-e0955.PMC10443761.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000000955","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Clinical sepsis phenotypes may be defined by a wide range of characteristics such as site of infection, organ dysfunction patterns, laboratory values, and demographics. There is a paucity of literature regarding the impact of site of infection on the timing and pattern of clinical sepsis markers. This study hypothesizes that important phenotypic variation in clinical markers and outcomes of sepsis exists when stratified by infection site.
Design: Retrospective cohort study.
Setting: Five hospitals within the Wake Forest Health System from June 2019 to December 2019.
Patients: Six thousand seven hundred fifty-three hospitalized adults with a discharge International Classification of Diseases, 10th Revision code for acute infection who met systemic inflammatory response syndrome (SIRS), quick Sepsis-related Organ Failure Assessment (qSOFA), or Sequential Organ Failure Assessment (SOFA) criteria during the index hospitalization.
Interventions: None.
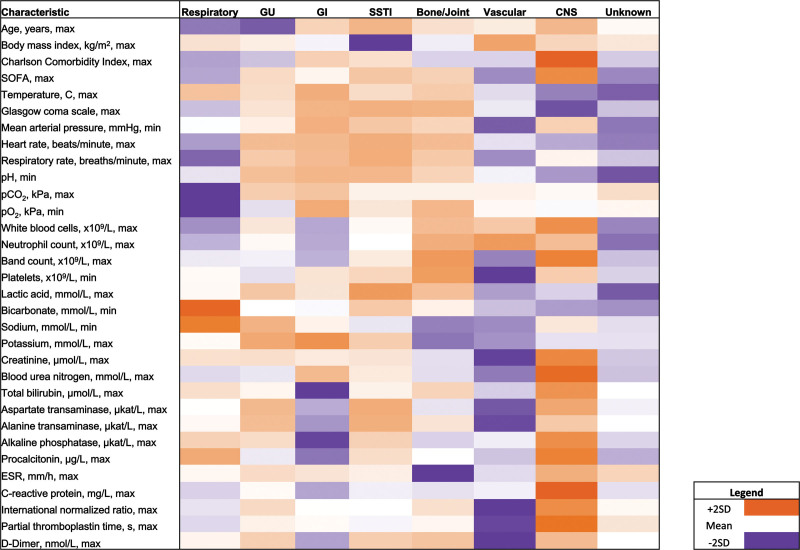
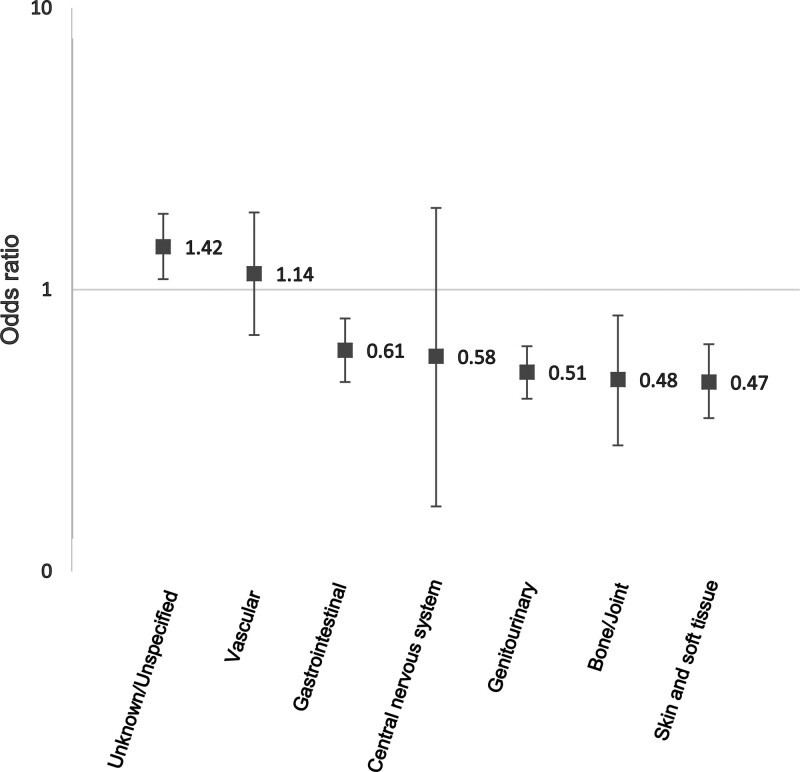
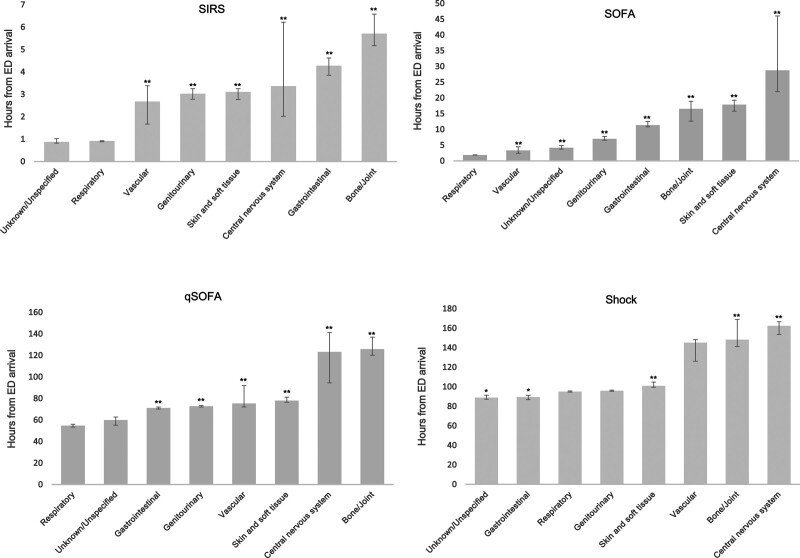
Measurements and main results: The primary outcome of interest was a composite of 30-day mortality or shock. Infection site was determined by a two-reviewer process. Significant demographic, vital sign, and laboratory result differences were seen across all infection sites. For the composite outcome of shock or 30-day mortality, unknown or unspecified infections had the highest proportion (21.34%) and CNS infections had the lowest proportion (8.11%). Respiratory, vascular, and unknown or unspecified infection sites showed a significantly increased adjusted and unadjusted odds of the composite outcome as compared with the other infection sites except CNS. Hospital time prior to SIRS positivity was shortest in unknown or unspecified infections at a median of 0.88 hours (interquartile range [IQR], 0.22-5.05 hr), and hospital time prior to qSOFA and SOFA positivity was shortest in respiratory infections at a median of 54.83 hours (IQR, 9.55-104.67 hr) and 1.88 hours (IQR, 0.47-17.40 hr), respectively.
Conclusions: Phenotypic variation in illness severity and mortality exists when stratified by infection site. There is a significantly higher adjusted and unadjusted odds of the composite outcome of 30-day mortality or shock in respiratory, vascular, and unknown or unspecified infections as compared with other sites.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
