{"title":"Ticagrelor or Clopidogrel as Antiplatelet Agents in Patients with Chronic Kidney Disease and Cardiovascular Disease: A Meta-analysis","authors":"Yinxue Guo, Pingyu Ge, Ziju Li, Jingxia Xiao, Lirui Xie","doi":"10.1007/s40256-023-00600-w","DOIUrl":null,"url":null,"abstract":"<div><h3>Introduction</h3><p>The worldwide prevalence of chronic kidney disease (CKD) has significantly increased in the past decades. Scientific reports have shown CKD to be an enhancing risk factor for the development of cardiovascular disease (CVD), which is the leading cause of premature death in patients with CKD. Clinical practice guidelines are ambiguous in view of the use of antiplatelet drugs in patients with CKD because patients with moderate-to-severe CKD were often excluded from clinical trials evaluating the efficacy and safety of anticoagulants and antiplatelet agents. In this analysis, we aimed to systematically assess the adverse cardiovascular and bleeding outcomes that were observed with ticagrelor versus clopidogrel use in patients with CKD and cardiovascular disease.</p><h3>Methods</h3><p>Electronic databases including Web of Science, Google Scholar, http://www.ClinicalTrials.gov, Cochrane database, EMBASE, and MEDLINE were carefully searched for English-based articles comparing ticagrelor with clopidogrel in patients with CKD. Adverse cardiovascular outcomes and bleeding events were the endpoints in this study. The latest version of the RevMan software (version 5.4) was used to analyze the data. Risk ratios (RR) with 95% confidence intervals (CI) were used to represent the data post analysis.</p><h3>Results</h3><p>A total of 15,664 participants were included in this analysis, whereby 2456 CKD participants were assigned to ticagrelor and 13,208 CKD participants were assigned to clopidogrel. Our current analysis showed that major adverse cardiac events (MACEs) (RR: 0.85, 95% CI: 0.71–1.03; <i>P</i> = 0.09), all-cause mortality (RR: 0.82, 95% CI: 0.57– 1.18; <i>P</i> = 0.29), cardiovascular death (RR: 0.83, 95% CI: 0.56–1.23; <i>P</i> = 0.35), myocardial infarction (RR: 0.87, 95% CI: 0.70–1.07; <i>P</i> = 0.19), ischemic stroke (RR: 0.80, 95% CI: 0.58–1.11; <i>P</i> = 0.18), and hemorrhagic stroke (RR: 1.06, 95% CI: 0.38–2.99; <i>P</i> = 0.91) were not significantly different in CKD patients who were treated with ticagrelor versus clopidogrel. Thrombolysis in myocardial infarction (TIMI)-defined minor (RR: 0.89, 95% CI: 0.52–1.53; <i>P</i> = 0.68) and TIMI major bleeding (RR: 1.10, 95% CI: 0.69–1.76; <i>P</i> = 0.67) were also not significantly different. However, bleeding defined according to the academic research consortium (BARC) bleeding type 1 or 2 (RR: 1.95, 95% CI: 1.13–3.37; <i>P</i> = 0.02) and BARC bleeding type 3 or 5 (RR: 1.70, 95% CI: 1.17–2.48; <i>P</i> = 0.006) were significantly higher with ticagrelor.</p><h3>Conclusions</h3><p>When compared with clopidogrel, even though ticagrelor was not associated with higher risk of adverse cardiovascular outcomes in these patients with CKD, it was associated with significantly higher BARC bleeding. Therefore, the safety outcomes of ticagrelor still require further evaluation in patients with CKD. Nevertheless, this hypothesis should only be confirmed with more powerful results that could usually only be achieved using large-scale randomized trials.</p></div>","PeriodicalId":7652,"journal":{"name":"American Journal of Cardiovascular Drugs","volume":"23 5","pages":"533 - 546"},"PeriodicalIF":3.0000,"publicationDate":"2023-08-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Cardiovascular Drugs","FirstCategoryId":"3","ListUrlMain":"https://link.springer.com/article/10.1007/s40256-023-00600-w","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
Introduction
The worldwide prevalence of chronic kidney disease (CKD) has significantly increased in the past decades. Scientific reports have shown CKD to be an enhancing risk factor for the development of cardiovascular disease (CVD), which is the leading cause of premature death in patients with CKD. Clinical practice guidelines are ambiguous in view of the use of antiplatelet drugs in patients with CKD because patients with moderate-to-severe CKD were often excluded from clinical trials evaluating the efficacy and safety of anticoagulants and antiplatelet agents. In this analysis, we aimed to systematically assess the adverse cardiovascular and bleeding outcomes that were observed with ticagrelor versus clopidogrel use in patients with CKD and cardiovascular disease.
Methods
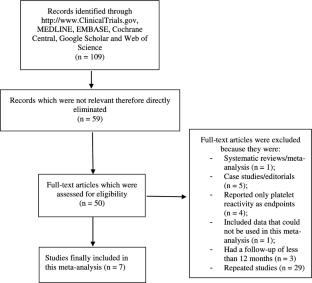
Electronic databases including Web of Science, Google Scholar, http://www.ClinicalTrials.gov, Cochrane database, EMBASE, and MEDLINE were carefully searched for English-based articles comparing ticagrelor with clopidogrel in patients with CKD. Adverse cardiovascular outcomes and bleeding events were the endpoints in this study. The latest version of the RevMan software (version 5.4) was used to analyze the data. Risk ratios (RR) with 95% confidence intervals (CI) were used to represent the data post analysis.
Results
A total of 15,664 participants were included in this analysis, whereby 2456 CKD participants were assigned to ticagrelor and 13,208 CKD participants were assigned to clopidogrel. Our current analysis showed that major adverse cardiac events (MACEs) (RR: 0.85, 95% CI: 0.71–1.03; P = 0.09), all-cause mortality (RR: 0.82, 95% CI: 0.57– 1.18; P = 0.29), cardiovascular death (RR: 0.83, 95% CI: 0.56–1.23; P = 0.35), myocardial infarction (RR: 0.87, 95% CI: 0.70–1.07; P = 0.19), ischemic stroke (RR: 0.80, 95% CI: 0.58–1.11; P = 0.18), and hemorrhagic stroke (RR: 1.06, 95% CI: 0.38–2.99; P = 0.91) were not significantly different in CKD patients who were treated with ticagrelor versus clopidogrel. Thrombolysis in myocardial infarction (TIMI)-defined minor (RR: 0.89, 95% CI: 0.52–1.53; P = 0.68) and TIMI major bleeding (RR: 1.10, 95% CI: 0.69–1.76; P = 0.67) were also not significantly different. However, bleeding defined according to the academic research consortium (BARC) bleeding type 1 or 2 (RR: 1.95, 95% CI: 1.13–3.37; P = 0.02) and BARC bleeding type 3 or 5 (RR: 1.70, 95% CI: 1.17–2.48; P = 0.006) were significantly higher with ticagrelor.
Conclusions
When compared with clopidogrel, even though ticagrelor was not associated with higher risk of adverse cardiovascular outcomes in these patients with CKD, it was associated with significantly higher BARC bleeding. Therefore, the safety outcomes of ticagrelor still require further evaluation in patients with CKD. Nevertheless, this hypothesis should only be confirmed with more powerful results that could usually only be achieved using large-scale randomized trials.
引言在过去的几十年里,全球慢性肾脏疾病(CKD)的患病率显著上升。科学报告表明,CKD是心血管疾病(CVD)发展的一个增强风险因素,心血管疾病是CKD患者过早死亡的主要原因。鉴于CKD患者使用抗血小板药物,临床实践指南并不明确,因为中重度CKD患者经常被排除在评估抗凝剂和抗血小板药物疗效和安全性的临床试验之外。在这项分析中,我们旨在系统评估在CKD和心血管疾病患者中使用替卡格雷与使用氯吡格雷观察到的不良心血管和出血结果。方法电子数据库包括Web of Science、Google Scholar、,http://www.ClinicalTrials.gov,Cochrane数据库、EMBASE和MEDLINE仔细搜索了比较CKD患者中替卡格雷和氯吡格雷的英文文章。不良心血管结局和出血事件是本研究的终点。最新版本的RevMan软件(5.4版)用于分析数据。风险比(RR)和95%置信区间(CI)用于表示分析后的数据。结果本分析共纳入15664名参与者,其中2456名CKD参与者被分配给替卡格雷,13208名CKD患者被分配给氯吡格雷。我们目前的分析显示,主要心脏不良事件(MACE)(RR:0.85,95%CI:0.71–1.03;P=0.09)、全因死亡率(RR:0.82,95%CI:0.57–1.18;P=0.29)、心血管死亡(RR:0.83,95%CI:0.56–1.23;P=0.35)、心肌梗死(RR:0.87,95%CI:0.70–1.07;P=0.19)、缺血性中风(RR:0.80,95%CI:0.58–1.11;P=0.18),和出血性卒中(RR:1.06,95%CI:0.38–2.99;P=0.91)在接受替卡格雷和氯吡格雷治疗的CKD患者中没有显著差异。定义为轻度心肌梗死(TIMI)的血栓溶解(RR:0.89,95%CI:0.52-1.53;P=0.68)和TIMI大出血(RR:1.10,95%CI:0.69-1.76;P=0.67)也没有显著差异。然而,根据学术研究联合会(BARC)定义的出血类型1或2(RR:1.95,95%CI:1.13–3.37;P=0.02)和BARC出血类型3或5(RR:1.70,95%CI:1.17–2.48;P=0.006),替卡格雷的出血显著更高。结论与氯吡格雷相比,尽管替卡格雷与这些CKD患者心血管不良后果的高风险无关,但它与明显更高的BARC出血有关。因此,替卡格雷的安全性结果仍需对CKD患者进行进一步评估。然而,这一假设只有通过更有力的结果才能得到证实,而这些结果通常只能通过大规模随机试验来实现。
期刊介绍:
Promoting rational therapy within the discipline of cardiology, the American Journal of Cardiovascular Drugs covers all aspects of the treatment of cardiovascular disorders, particularly the place in therapy of newer and established agents.
Via a program of reviews and original clinical research articles, the journal addresses major issues relating to treatment of these disorders, including the pharmacology, efficacy and adverse effects of the major classes of drugs; information on newly developed drugs and drug classes; the therapeutic implications of latest research into the aetiology of cardiovascular disorders; and the practical management of specific clinical situations.
The American Journal of Cardiovascular Drugs offers a range of additional enhanced features designed to increase the visibility, readership and educational value of the journal’s content. Each article is accompanied by a Key Points summary, giving a time-efficient overview of the content to a wide readership. Articles may be accompanied by plain language summaries to assist patients, caregivers and others in understanding important medical advances. The journal also provides the option to include various other types of enhanced features including slide sets, videos and animations. All enhanced features are peer reviewed to the same high standard as the article itself. Peer review is conducted using Editorial Manager®, supported by a database of international experts. This database is shared with other Adis journals.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
