{"title":"Refined Diagnostic Protocol for Diabetic Polyneuropathy: Paving the Way for Timely Detection.","authors":"Byung-Mo Oh","doi":"10.5535/arm.23122","DOIUrl":null,"url":null,"abstract":"This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/ licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited. I carefully studied the proposal from Lee et al. [1] describing a nerve conduction study (NCS) algorithm for grading the severity of diabetic distal symmetric sensorimotor polyneuropathy (DSPN). Despite the article’s brevity, it was evident that the authors put substantial effort into research and contemplation on the topic. Henceforth, I will refer to this diagnostic NCS algorithm as “Lee’s Severity System” or “Lee’s algorithm.” In 2020, the estimated prevalence of diabetes mellitus among Korean adults was 16.7% [2]. Diabetic neuropathy, which affects approximately one-third of the patients with type 1 or type 2 diabetes, increases the risk of painless foot ulcers leading to amputations [3]. Although the NCS is the most comprehensive and accurate diagnostic tool for DSPN, it is not routinely integrated into standard clinical care for diabetic patients. This reluctance is understandable; without concrete evidence that NCS enhances clinical outcomes, the associated costs, time commitments, and potential patient discomfort might deter clinicians. In this regard, Lee’s algorithm is primarily efficient, offering several advantages. Using this algorithm, NCS of the lower extremities that are more vulnerable at an earlier stage of DSPN can be first performed. If these results are within normal limits, the examination can be completed with only a tibial F-wave study in the contralateral lower limb. In addition, Lee’s algorithm suggests that the contralateral lower extremity or non-dominant upper extremity can be examined only when there is an additional need. Taken together, Lee’s Severity System has the potential to significantly reduce the NCS examination time, especially in patients with early-stage to mild DSPN. Applying these streamlined algorithms will minimize the time, cost, and discomfort associated with NCS, allowing its application to most patients with diabetes. The NCS is more sensitive than the Semmes-Weinstein monofilament test and can comprehensively assess the entire sensory and motor systems. It would greatly benefit if the NCS could be completed in as little as 30 minutes. Lee’s Severity System employs an ordinal scale that classifies DSPN severity into five stages based on NCS outcomes. This framework offers significant clinical utility, presenting a nuanced understanding of disease severity rather than a simple binary diagnosis of the presence or absence of DSPN. Furthermore, it identifies “early stage” DSPN, potentially a pivotal therapeutic juncture. Baba et al. introduced a comparable DSPN severity scale [4]. The mild, moderate, and severe grades in Lee’s Severity System mirror grades 2, 3, and 4 of Baba’s classification, diagnosRefined Diagnostic Protocol for Diabetic Polyneuropathy: Paving the Way for Timely Detection","PeriodicalId":47738,"journal":{"name":"Annals of Rehabilitation Medicine-ARM","volume":"47 4","pages":"234-236"},"PeriodicalIF":2.9000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a8/46/arm-23122.PMC10475809.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Rehabilitation Medicine-ARM","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5535/arm.23122","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"REHABILITATION","Score":null,"Total":0}
引用次数: 0
Abstract
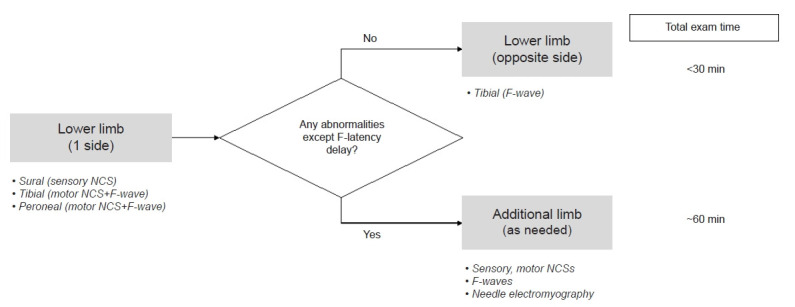
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/ licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited. I carefully studied the proposal from Lee et al. [1] describing a nerve conduction study (NCS) algorithm for grading the severity of diabetic distal symmetric sensorimotor polyneuropathy (DSPN). Despite the article’s brevity, it was evident that the authors put substantial effort into research and contemplation on the topic. Henceforth, I will refer to this diagnostic NCS algorithm as “Lee’s Severity System” or “Lee’s algorithm.” In 2020, the estimated prevalence of diabetes mellitus among Korean adults was 16.7% [2]. Diabetic neuropathy, which affects approximately one-third of the patients with type 1 or type 2 diabetes, increases the risk of painless foot ulcers leading to amputations [3]. Although the NCS is the most comprehensive and accurate diagnostic tool for DSPN, it is not routinely integrated into standard clinical care for diabetic patients. This reluctance is understandable; without concrete evidence that NCS enhances clinical outcomes, the associated costs, time commitments, and potential patient discomfort might deter clinicians. In this regard, Lee’s algorithm is primarily efficient, offering several advantages. Using this algorithm, NCS of the lower extremities that are more vulnerable at an earlier stage of DSPN can be first performed. If these results are within normal limits, the examination can be completed with only a tibial F-wave study in the contralateral lower limb. In addition, Lee’s algorithm suggests that the contralateral lower extremity or non-dominant upper extremity can be examined only when there is an additional need. Taken together, Lee’s Severity System has the potential to significantly reduce the NCS examination time, especially in patients with early-stage to mild DSPN. Applying these streamlined algorithms will minimize the time, cost, and discomfort associated with NCS, allowing its application to most patients with diabetes. The NCS is more sensitive than the Semmes-Weinstein monofilament test and can comprehensively assess the entire sensory and motor systems. It would greatly benefit if the NCS could be completed in as little as 30 minutes. Lee’s Severity System employs an ordinal scale that classifies DSPN severity into five stages based on NCS outcomes. This framework offers significant clinical utility, presenting a nuanced understanding of disease severity rather than a simple binary diagnosis of the presence or absence of DSPN. Furthermore, it identifies “early stage” DSPN, potentially a pivotal therapeutic juncture. Baba et al. introduced a comparable DSPN severity scale [4]. The mild, moderate, and severe grades in Lee’s Severity System mirror grades 2, 3, and 4 of Baba’s classification, diagnosRefined Diagnostic Protocol for Diabetic Polyneuropathy: Paving the Way for Timely Detection



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
