Alessandro Aprato, Luigi Branca Vergano, Alessandro Casiraghi, Francesco Liuzza, Umberto Mezzadri, Alberto Balagna, Lorenzo Prandoni, Mohamed Rohayem, Lorenzo Sacchi, Amarildo Smakaj, Mario Arduini, Alessandro Are, Concetto Battiato, Marco Berlusconi, Federico Bove, Stefano Cattaneo, Matteo Cavanna, Federico Chiodini, Matteo Commessatti, Francesco Addevico, Rocco Erasmo, Alberto Ferreli, Claudio Galante, Pietro Domenico Giorgi, Federico Lamponi, Alessandro Moghnie, Michel Oransky, Antonio Panella, Raffaele Pascarella, Federico Santolini, Giuseppe Rosario Schiro, Marco Stella, Kristijan Zoccola, Alessandro Massé
{"title":"Consensus for management of sacral fractures: from the diagnosis to the treatment, with a focus on the role of decompression in sacral fractures.","authors":"Alessandro Aprato, Luigi Branca Vergano, Alessandro Casiraghi, Francesco Liuzza, Umberto Mezzadri, Alberto Balagna, Lorenzo Prandoni, Mohamed Rohayem, Lorenzo Sacchi, Amarildo Smakaj, Mario Arduini, Alessandro Are, Concetto Battiato, Marco Berlusconi, Federico Bove, Stefano Cattaneo, Matteo Cavanna, Federico Chiodini, Matteo Commessatti, Francesco Addevico, Rocco Erasmo, Alberto Ferreli, Claudio Galante, Pietro Domenico Giorgi, Federico Lamponi, Alessandro Moghnie, Michel Oransky, Antonio Panella, Raffaele Pascarella, Federico Santolini, Giuseppe Rosario Schiro, Marco Stella, Kristijan Zoccola, Alessandro Massé","doi":"10.1186/s10195-023-00726-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is no evidence in the current literature about the best treatment option in sacral fracture with or without neurological impairment.</p><p><strong>Materials and methods: </strong>The Italian Pelvic Trauma Association (A.I.P.) decided to organize a consensus to define the best treatment for traumatic and insufficiency fractures according to neurological impairment.</p><p><strong>Results: </strong>Consensus has been reached for the following statements: When complete neurological examination cannot be performed, pelvic X-rays, CT scan, hip and pelvis MRI, lumbosacral MRI, and lower extremities evoked potentials are useful. Lower extremities EMG should not be used in an acute setting; a patient with cauda equina syndrome associated with a sacral fracture represents an absolute indication for sacral reduction and the correct timing for reduction is \"as early as possible\". An isolated and incomplete radicular neurological deficit of the lower limbs does not represent an indication for laminectomy after reduction in the case of a displaced sacral fracture in a high-energy trauma, while a worsening and progressive radicular neurological deficit represents an indication. In the case of a displaced sacral fracture and neurological deficit with imaging showing no evidence of nerve root compression, a laminectomy after reduction is not indicated. In a patient who was not initially investigated from a neurological point of view, if a clinical investigation conducted after 72 h identifies a neurological deficit in the presence of a displaced sacral fracture with nerve compression on MRI, a laminectomy after reduction may be indicated. In the case of an indication to perform a sacral decompression, a first attempt with closed reduction through external manoeuvres is not mandatory. Transcondylar traction does not represent a valid method for performing a closed decompression. Following a sacral decompression, a sacral fixation (e.g. sacroiliac screw, triangular osteosynthesis, lumbopelvic fixation) should be performed. An isolated and complete radicular neurological deficit of the lower limbs represents an indication for laminectomy after reduction in the case of a displaced sacral fracture in a low-energy trauma associated with imaging suggestive of root compression. An isolated and incomplete radicular neurological deficit of the lower limbs does not represent an absolute indication. A worsening and progressive radicular neurological deficit of the lower limbs represents an indication for laminectomy after reduction in the case of a displaced sacral fracture in a low-energy trauma associated with imaging suggestive of root compression. In the case of a displaced sacral fracture and neurological deficit in a low-energy trauma, sacral decompression followed by surgical fixation is indicated.</p><p><strong>Conclusions: </strong>This consensus collects expert opinion about this topic and may guide the surgeon in choosing the best treatment for these patients.</p><p><strong>Level of evidence: </strong>IV.</p><p><strong>Trial registration: </strong>not applicable (consensus paper).</p>","PeriodicalId":48603,"journal":{"name":"Journal of Orthopaedics and Traumatology","volume":"24 1","pages":"46"},"PeriodicalIF":3.7000,"publicationDate":"2023-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10477162/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Orthopaedics and Traumatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s10195-023-00726-2","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There is no evidence in the current literature about the best treatment option in sacral fracture with or without neurological impairment.
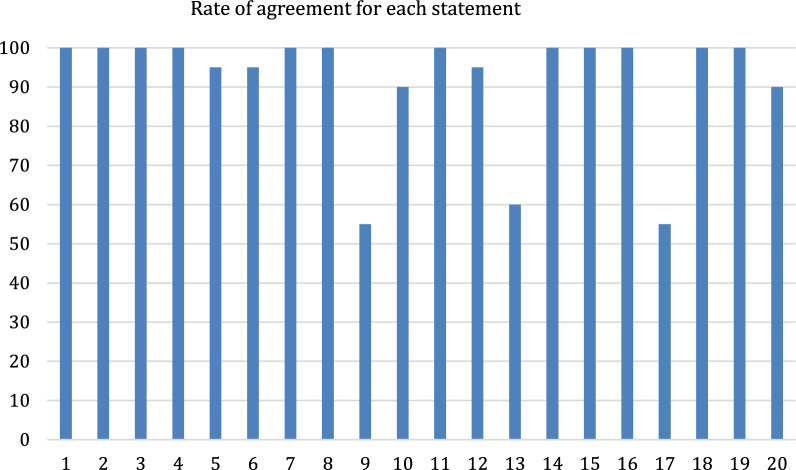
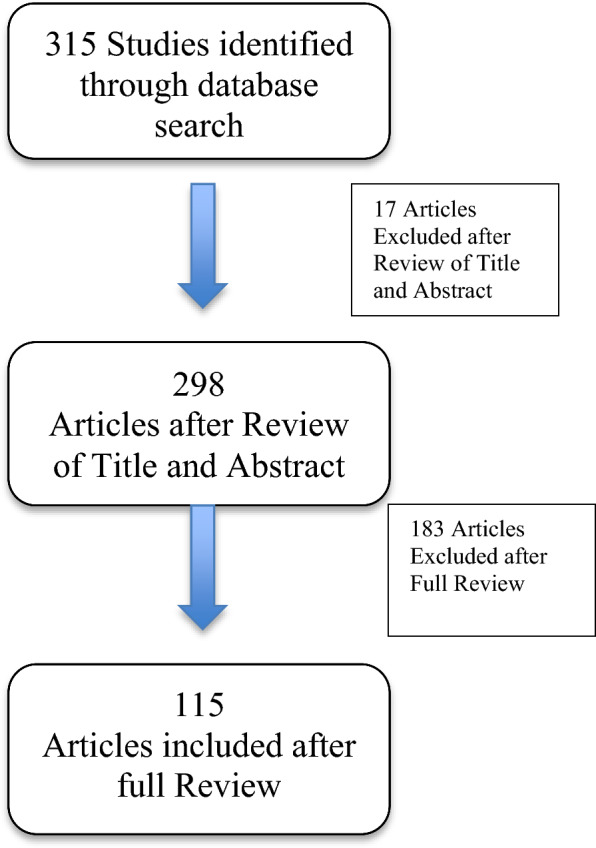
Materials and methods: The Italian Pelvic Trauma Association (A.I.P.) decided to organize a consensus to define the best treatment for traumatic and insufficiency fractures according to neurological impairment.
Results: Consensus has been reached for the following statements: When complete neurological examination cannot be performed, pelvic X-rays, CT scan, hip and pelvis MRI, lumbosacral MRI, and lower extremities evoked potentials are useful. Lower extremities EMG should not be used in an acute setting; a patient with cauda equina syndrome associated with a sacral fracture represents an absolute indication for sacral reduction and the correct timing for reduction is "as early as possible". An isolated and incomplete radicular neurological deficit of the lower limbs does not represent an indication for laminectomy after reduction in the case of a displaced sacral fracture in a high-energy trauma, while a worsening and progressive radicular neurological deficit represents an indication. In the case of a displaced sacral fracture and neurological deficit with imaging showing no evidence of nerve root compression, a laminectomy after reduction is not indicated. In a patient who was not initially investigated from a neurological point of view, if a clinical investigation conducted after 72 h identifies a neurological deficit in the presence of a displaced sacral fracture with nerve compression on MRI, a laminectomy after reduction may be indicated. In the case of an indication to perform a sacral decompression, a first attempt with closed reduction through external manoeuvres is not mandatory. Transcondylar traction does not represent a valid method for performing a closed decompression. Following a sacral decompression, a sacral fixation (e.g. sacroiliac screw, triangular osteosynthesis, lumbopelvic fixation) should be performed. An isolated and complete radicular neurological deficit of the lower limbs represents an indication for laminectomy after reduction in the case of a displaced sacral fracture in a low-energy trauma associated with imaging suggestive of root compression. An isolated and incomplete radicular neurological deficit of the lower limbs does not represent an absolute indication. A worsening and progressive radicular neurological deficit of the lower limbs represents an indication for laminectomy after reduction in the case of a displaced sacral fracture in a low-energy trauma associated with imaging suggestive of root compression. In the case of a displaced sacral fracture and neurological deficit in a low-energy trauma, sacral decompression followed by surgical fixation is indicated.
Conclusions: This consensus collects expert opinion about this topic and may guide the surgeon in choosing the best treatment for these patients.
Level of evidence: IV.
Trial registration: not applicable (consensus paper).
期刊介绍:
The Journal of Orthopaedics and Traumatology, the official open access peer-reviewed journal of the Italian Society of Orthopaedics and Traumatology, publishes original papers reporting basic or clinical research in the field of orthopaedic and traumatologic surgery, as well as systematic reviews, brief communications, case reports and letters to the Editor. Narrative instructional reviews and commentaries to original articles may be commissioned by Editors from eminent colleagues. The Journal of Orthopaedics and Traumatology aims to be an international forum for the communication and exchange of ideas concerning the various aspects of orthopaedics and musculoskeletal trauma.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
