{"title":"Computed tomography angiographic study of surgical anatomy of thyroid arteries: Clinical implications in neck dissection.","authors":"Yashu Bhardwaj, Brijendra Singh, Pooja Bhadoria, Rashmi Malhotra, Swarnava Tarafdar, Kanchan Bisht","doi":"10.4329/wjr.v15.i6.182","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The course and variations of thyroid arteries must be understood by surgeons to prevent bleeding during operative procedures of the thyroid gland. There is limited scientific literature regarding the radiological anatomy of thyroid arteries in this geographical area, the Garhwal region of Sub-Himalayan belt, which is considered to be the endemic belt of goiter. Computed tomography angiography provides a three-dimensional orientation of the vascular and surgical anatomy of the entire cervical region.</p><p><strong>Aim: </strong>To estimate the proportion of variation in origin of thyroid arteries using Computed Tomography Angiography.</p><p><strong>Methods: </strong>Using Computed Tomography Angiography, the presence and origin of the superior thyroid artery, inferior thyroid artery, and thyroid ima artery were observed and assessed.</p><p><strong>Results: </strong>Out of total 210 subjects, superior thyroid artery was seen to be emerging from external carotid artery in 77.1% cases. The artery was found to be originating at the level of bifurcation of common carotid artery in 14.3% cases, whereas in 8.6% cases, it emerged as a direct branch of the common carotid artery. Similarly, the inferior thyroid artery was observed to be emerging from thyrocervical trunk, subclavian artery and vertebral artery in 95.7% cases, 3.3% and 1% cases, respectively. Thyroid ima artery was also reported in a subject, arising from the brachiocephalic trunk.</p><p><strong>Conclusion: </strong>To avoid vascular injuries, excessive and uncontrollable bleeding, intra-operative difficulties, and post-operative issues, it is imperative for surgeons to be aware of the course and variations of thyroid arteries.</p>","PeriodicalId":23819,"journal":{"name":"World journal of radiology","volume":"15 6","pages":"182-190"},"PeriodicalIF":1.5000,"publicationDate":"2023-06-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c3/7d/WJR-15-182.PMC10324493.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World journal of radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4329/wjr.v15.i6.182","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The course and variations of thyroid arteries must be understood by surgeons to prevent bleeding during operative procedures of the thyroid gland. There is limited scientific literature regarding the radiological anatomy of thyroid arteries in this geographical area, the Garhwal region of Sub-Himalayan belt, which is considered to be the endemic belt of goiter. Computed tomography angiography provides a three-dimensional orientation of the vascular and surgical anatomy of the entire cervical region.
Aim: To estimate the proportion of variation in origin of thyroid arteries using Computed Tomography Angiography.
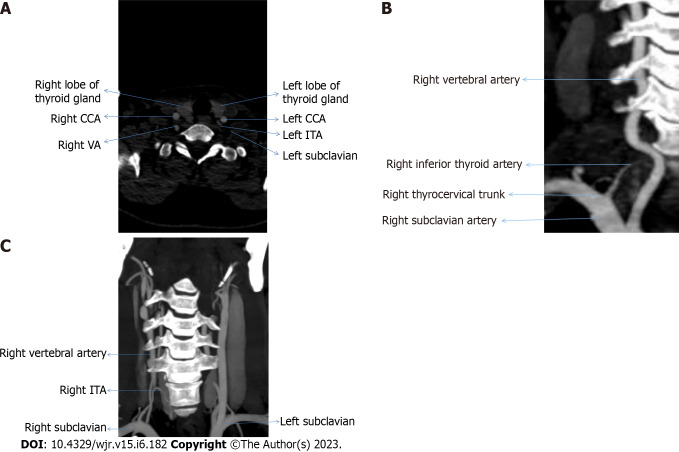
Methods: Using Computed Tomography Angiography, the presence and origin of the superior thyroid artery, inferior thyroid artery, and thyroid ima artery were observed and assessed.
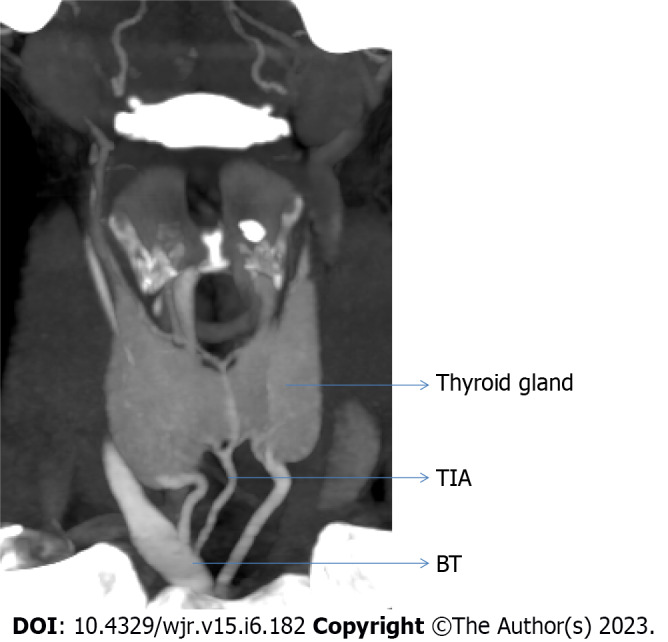
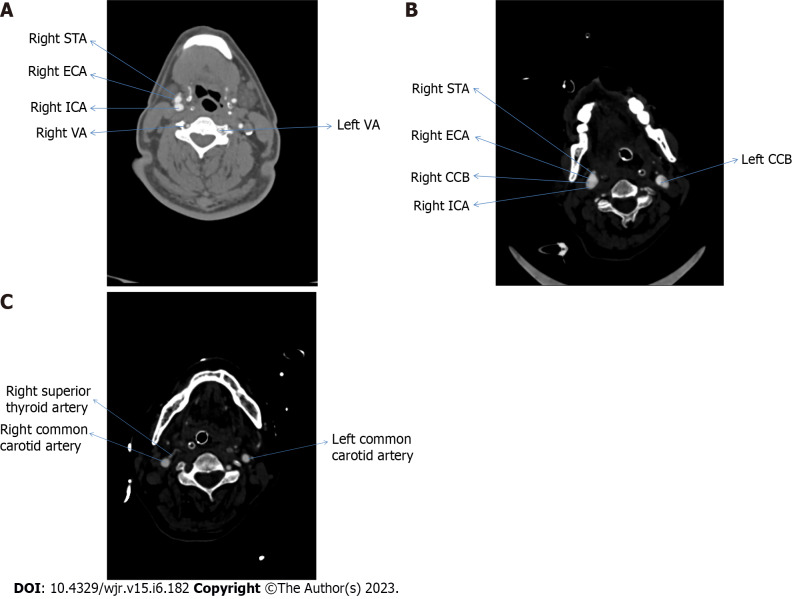
Results: Out of total 210 subjects, superior thyroid artery was seen to be emerging from external carotid artery in 77.1% cases. The artery was found to be originating at the level of bifurcation of common carotid artery in 14.3% cases, whereas in 8.6% cases, it emerged as a direct branch of the common carotid artery. Similarly, the inferior thyroid artery was observed to be emerging from thyrocervical trunk, subclavian artery and vertebral artery in 95.7% cases, 3.3% and 1% cases, respectively. Thyroid ima artery was also reported in a subject, arising from the brachiocephalic trunk.
Conclusion: To avoid vascular injuries, excessive and uncontrollable bleeding, intra-operative difficulties, and post-operative issues, it is imperative for surgeons to be aware of the course and variations of thyroid arteries.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
