{"title":"Resection of high-grade glioma involving language areas assisted by multimodal techniques under general anesthesia: a retrospective study.","authors":"Meng Cui, Yukun Liu, Chunhui Zhou, Hewen Chen, Xin Gao, Jiayu Liu, Qingbao Guo, Bing Guan, Xiaodong Ma","doi":"10.1186/s41016-023-00340-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Multimodal techniques-assisted resection of glioma under general anesthesia (GA) has been shown to achieve similar clinical outcomes as awake craniotomy (AC) in some studies. In this study, we aim to validate the use of multimodal techniques can achieve the maximal safe resection of high-grade glioma involving language areas (HGILAs) under GA.</p><p><strong>Methods: </strong>HGILAs cases were reviewed and collected between January 2009 and December 2020 in our center. Patients were separated into multimodal group (using neuronavigation, intraoperative MRI combined with direct electrical stimulation [DES] and neuromonitoring [IONM]) and conventional group (neuronavigation alone) and clinical outcomes were compared between groups. Studies of HGILAs were reviewed systematically and the meta-analysis results of previous (GA or AC) studies were compared with our results.</p><p><strong>Results: </strong>Finally, there were 263 patients in multimodal group and 137 patients in conventional group. Compared to the conventional group, the multimodal group achieved the higher median EOR (100% versus 94.32%, P < 0.001) and rate of gross total resection (GTR) (73.8% versus 36.5%, P < 0.001) and the lower incidence of permanent language deficit (PLD) (9.5% versus 19.7%, P = 0.004). The multimodal group achieved the longer median PFS (16.8 versus 10.3 months, P < 0.001) and OS (23.7 versus 15.7 months, P < 0.001) than the conventional group. The multimodal group achieved a higher rate of GTR than the cohorts in previous multimodal studies under GA and AC (73.8% versus 55.7% [95%CI 32.0-79.3%] versus 53.4% [35.5-71.2%]). The multimodal group had a lower incidence of PLD than the cohorts in previous multimodal studies under GA (9.5% versus 14.0% [5.8-22.1%]) and our incidence of PLD was a little higher than that of previous multimodal studies under AC (9.5% versus 7.5% [3.7-11.2%]). Our multimodal group also achieved a relative longer survival than previous studies.</p><p><strong>Conclusions: </strong>Surgery assisted by multimodal techniques can achieve maximal safe resection for HGILAs under GA. Further prospective studies are needed to compare GA with AC for HGILAs.</p>","PeriodicalId":36700,"journal":{"name":"Chinese Neurosurgical Journal","volume":"9 1","pages":"25"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10494413/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chinese Neurosurgical Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s41016-023-00340-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Multimodal techniques-assisted resection of glioma under general anesthesia (GA) has been shown to achieve similar clinical outcomes as awake craniotomy (AC) in some studies. In this study, we aim to validate the use of multimodal techniques can achieve the maximal safe resection of high-grade glioma involving language areas (HGILAs) under GA.
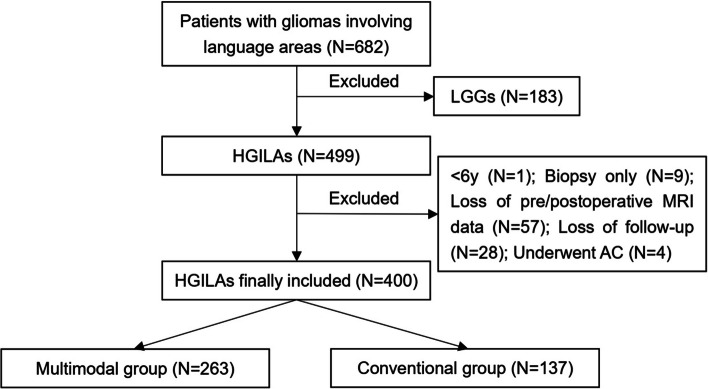
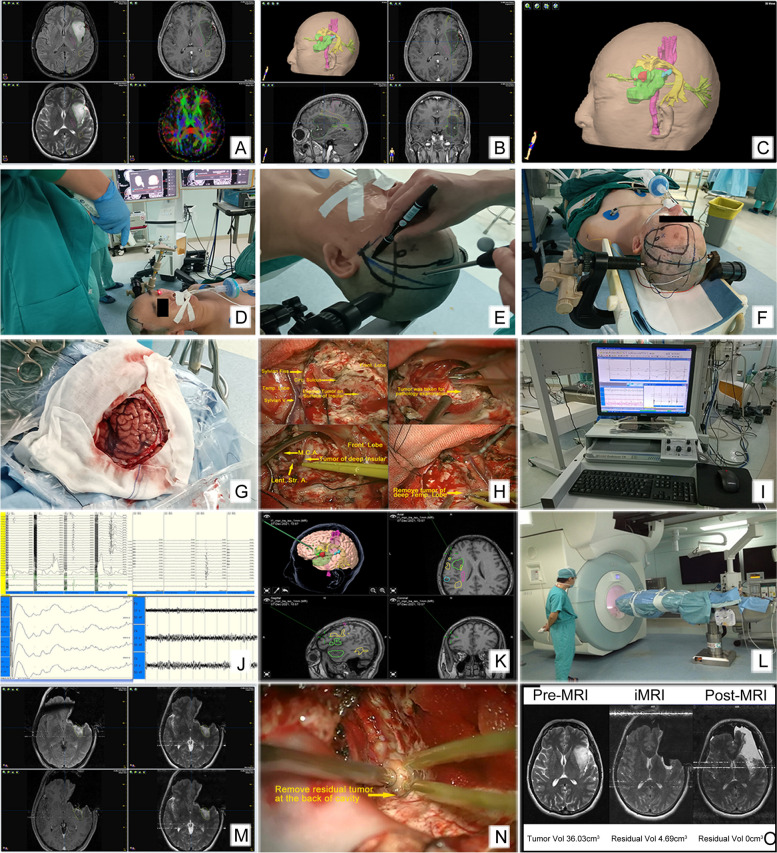
Methods: HGILAs cases were reviewed and collected between January 2009 and December 2020 in our center. Patients were separated into multimodal group (using neuronavigation, intraoperative MRI combined with direct electrical stimulation [DES] and neuromonitoring [IONM]) and conventional group (neuronavigation alone) and clinical outcomes were compared between groups. Studies of HGILAs were reviewed systematically and the meta-analysis results of previous (GA or AC) studies were compared with our results.
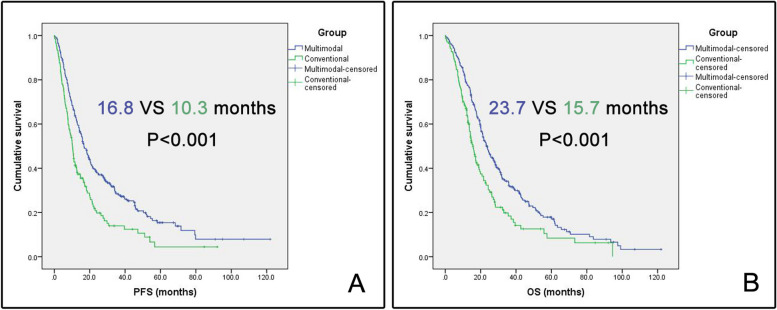
Results: Finally, there were 263 patients in multimodal group and 137 patients in conventional group. Compared to the conventional group, the multimodal group achieved the higher median EOR (100% versus 94.32%, P < 0.001) and rate of gross total resection (GTR) (73.8% versus 36.5%, P < 0.001) and the lower incidence of permanent language deficit (PLD) (9.5% versus 19.7%, P = 0.004). The multimodal group achieved the longer median PFS (16.8 versus 10.3 months, P < 0.001) and OS (23.7 versus 15.7 months, P < 0.001) than the conventional group. The multimodal group achieved a higher rate of GTR than the cohorts in previous multimodal studies under GA and AC (73.8% versus 55.7% [95%CI 32.0-79.3%] versus 53.4% [35.5-71.2%]). The multimodal group had a lower incidence of PLD than the cohorts in previous multimodal studies under GA (9.5% versus 14.0% [5.8-22.1%]) and our incidence of PLD was a little higher than that of previous multimodal studies under AC (9.5% versus 7.5% [3.7-11.2%]). Our multimodal group also achieved a relative longer survival than previous studies.
Conclusions: Surgery assisted by multimodal techniques can achieve maximal safe resection for HGILAs under GA. Further prospective studies are needed to compare GA with AC for HGILAs.
背景:在一些研究中,全麻(GA)下的多模式技术辅助胶质瘤切除术已被证明与清醒开颅术(AC)取得相似的临床结果。在这项研究中,我们的目的是验证使用多模式技术可以在GA下实现涉及语言区(HGILAs)的高级别胶质瘤的最大安全切除。方法:对2009年1月至2020年12月在我中心收集的HGILAs病例进行回顾性分析。将患者分为多模式组(使用神经导航、术中MRI联合直接电刺激[DES]和神经监测[IONM])和常规组(单独使用神经导航),比较两组临床结果。我们系统地回顾了HGILAs的研究,并将以往(GA或AC)研究的meta分析结果与我们的结果进行了比较。结果:多模式组263例,常规组137例。与常规组相比,多模式组的中位EOR更高(100% vs 94.32%), P结论:多模式技术辅助下的手术可以实现GA下HGILAs的最大安全切除。需要进一步的前瞻性研究来比较GA和AC对HGILAs的影响。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
