{"title":"Neuropathies Following an Ultrasound-Guided Axillary Brachial Plexus Block.","authors":"Keito Koh, Onishi Tatsuki, Sonoko Sakuraba, Sho Yamazaki, Hajime Yako, Takeshi Omae","doi":"10.2147/LRA.S426515","DOIUrl":null,"url":null,"abstract":"Purpose Ultrasound-guided brachial plexus block (UGBPB) has interscalene, supraclavicular, infraclavicular, and axillary approaches. The axillary block is considered to be the safest and with fewer adverse events compared to the interscalene (eg, phrenic nerve block, spinal cord or vertebral artery puncture) and supraclavicular (eg, pneumothorax). However, with regard to postoperative neurological symptoms (PONS), it is controversial whether its incidence after an axillary block was higher than that after non-axillary approaches”. In this study, we investigated whether the incidence of a neuropathy after an axillary block was higher than that after non-axillary approaches. Patients and Methods This was a single-center, retrospective cohort study. All UGBPBs were performed under general anesthesia between January 2014 and March 2020. The outcomes included the overall incidence of PONS and neuropathies for axillary and non-axillary approaches. The etiology, symptoms, and outcomes of patients were investigated. Results Of the 992 patients, 143 (14%) and 849 (86%) were subjected to axillary and non-axillary approaches, respectively. Among 19 cases (19.2:1000; 95% confidence interval [CI], 18.2–20.1) of PONS, four (4.0:1000; 95% CI, 3.8–4.2) were neuropathies attributed to the UGBPB, three (21.0:1000; 95% CI, 18.1–23.8) to the axillary and one (2.8:1000; 95% CI, 2.6–3.1) to non-axillary approaches. The incidence of neuropathies after an axillary block was significantly higher than that after non-axillary approaches (P = 0.005). Conclusion The incidence of neuropathies after US-guided axillary block under general anesthesia was significantly higher than that after non-axillary approaches.","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"16 ","pages":"123-132"},"PeriodicalIF":1.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/92/b4/lra-16-123.PMC10488563.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S426515","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
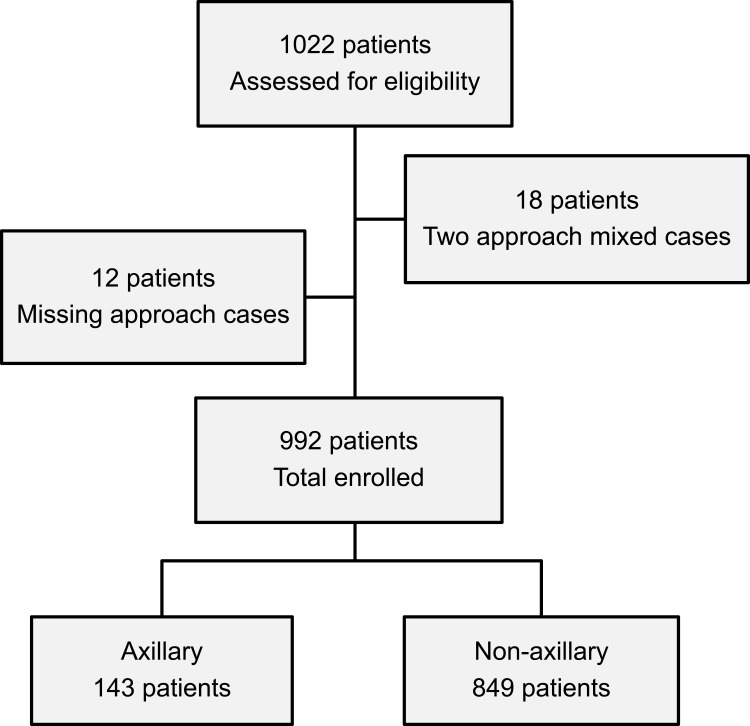
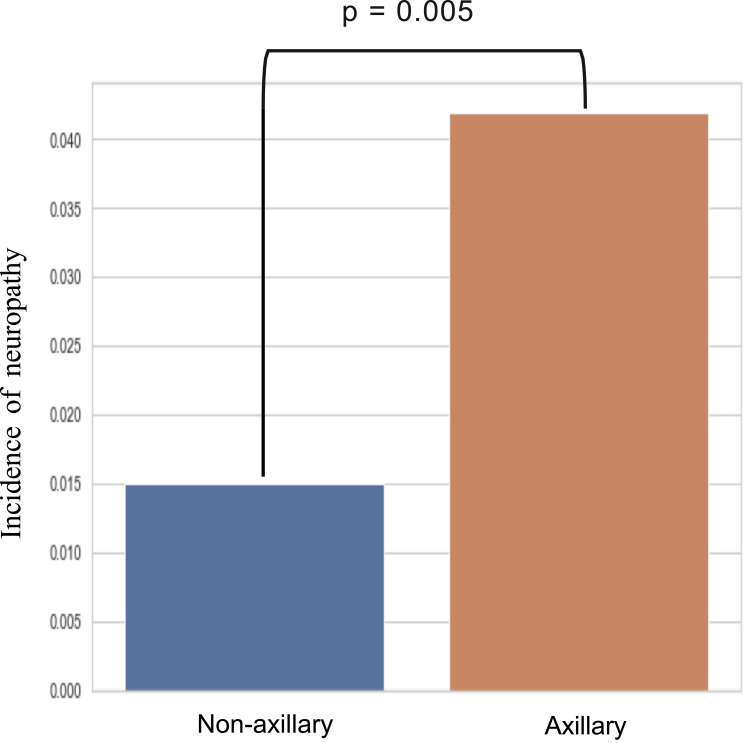
Purpose Ultrasound-guided brachial plexus block (UGBPB) has interscalene, supraclavicular, infraclavicular, and axillary approaches. The axillary block is considered to be the safest and with fewer adverse events compared to the interscalene (eg, phrenic nerve block, spinal cord or vertebral artery puncture) and supraclavicular (eg, pneumothorax). However, with regard to postoperative neurological symptoms (PONS), it is controversial whether its incidence after an axillary block was higher than that after non-axillary approaches”. In this study, we investigated whether the incidence of a neuropathy after an axillary block was higher than that after non-axillary approaches. Patients and Methods This was a single-center, retrospective cohort study. All UGBPBs were performed under general anesthesia between January 2014 and March 2020. The outcomes included the overall incidence of PONS and neuropathies for axillary and non-axillary approaches. The etiology, symptoms, and outcomes of patients were investigated. Results Of the 992 patients, 143 (14%) and 849 (86%) were subjected to axillary and non-axillary approaches, respectively. Among 19 cases (19.2:1000; 95% confidence interval [CI], 18.2–20.1) of PONS, four (4.0:1000; 95% CI, 3.8–4.2) were neuropathies attributed to the UGBPB, three (21.0:1000; 95% CI, 18.1–23.8) to the axillary and one (2.8:1000; 95% CI, 2.6–3.1) to non-axillary approaches. The incidence of neuropathies after an axillary block was significantly higher than that after non-axillary approaches (P = 0.005). Conclusion The incidence of neuropathies after US-guided axillary block under general anesthesia was significantly higher than that after non-axillary approaches.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
