Okong Doreen Alaleit , Jonathan Kajjimu , Kalanzi Joseph , Magara Stella Namirembe , Peter K. Agaba , Andrew Kintu
{"title":"Description and analysis of the emergency obstetric interfacility ambulance transfers (IFTs) to Kawempe National Referral Hospital in Uganda","authors":"Okong Doreen Alaleit , Jonathan Kajjimu , Kalanzi Joseph , Magara Stella Namirembe , Peter K. Agaba , Andrew Kintu","doi":"10.1016/j.afjem.2023.06.003","DOIUrl":null,"url":null,"abstract":"<div><h3>Introduction</h3><p>In Uganda, 2% of women die from maternal causes with a mortality rate of 336 maternal deaths per 100,000 live births. According to the World Health Organization Uganda is one of the top three contributors to maternal mortality in sub-Saharan Africa. Uganda has parallel weak ambulance systems, government, and non-government-owned, that transport obstetric emergencies to higher-level facilities. These two operations lack standards of medical care and inter-facility transfer (IFT) protocols to direct care. Limited studies exist which assess the state of Emergency Care Services in Uganda and none has been performed to assess the ambulance referral services utilized to address obstetric emergencies.</p></div><div><h3>Objective</h3><p>The present study was performed to describe the ambulance transfer processes of obstetric emergencies by analyzing cases arriving at Kawempe National Referral Hospital (KNRH) from outlying health facilities</p></div><div><h3>Methods</h3><p>The study was based at KNRH in Kampala, Uganda. It was a descriptive and analytic cross-sectional study. Trained research assistants enrolled participating patients who met the inclusion criteria consecutively on arrival by ambulance at the hospital. Utilizing a questionnaire, quantitative data was collected from the ambulance driver, the sending facility referral form, and the receiving hospital's ambulance log book for each case. The sample size was 215.</p></div><div><h3>Results</h3><p>The median age was 27 years and the majority of patients were referred because of hypertensive disorders (34.9%), obstructed labor (26.5%) and hemorrhage (20.9%). The median total response time for transfer of obstetric emergencies was 50 min, from ambulance activation until the mother was received at KNRH. Differences were identified between government and non-government-owned ambulances in regards to the method of activation, medical escort staffing, number of vital signs recorded, and ambulance onboard medical care. Ambulances parked at the facility took the shortest transfer time and EMT-supported ambulances had the greatest number of vital signs taken<strong>.</strong></p></div><div><h3>Conclusions</h3><p>Recommendations are to develop an integrated ambulance system for both government and non-government ambulances with standards especially in regards to standardized scripted call-center calls analysis, dispatch activation time, response-to-patient time, and trained ambulance professional staffing and medical care whenever in patient transport mode.</p></div>","PeriodicalId":48515,"journal":{"name":"African Journal of Emergency Medicine","volume":"13 3","pages":"Pages 183-190"},"PeriodicalIF":1.2000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10359711/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"African Journal of Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2211419X23000319","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 1
Abstract
Introduction
In Uganda, 2% of women die from maternal causes with a mortality rate of 336 maternal deaths per 100,000 live births. According to the World Health Organization Uganda is one of the top three contributors to maternal mortality in sub-Saharan Africa. Uganda has parallel weak ambulance systems, government, and non-government-owned, that transport obstetric emergencies to higher-level facilities. These two operations lack standards of medical care and inter-facility transfer (IFT) protocols to direct care. Limited studies exist which assess the state of Emergency Care Services in Uganda and none has been performed to assess the ambulance referral services utilized to address obstetric emergencies.
Objective
The present study was performed to describe the ambulance transfer processes of obstetric emergencies by analyzing cases arriving at Kawempe National Referral Hospital (KNRH) from outlying health facilities
Methods
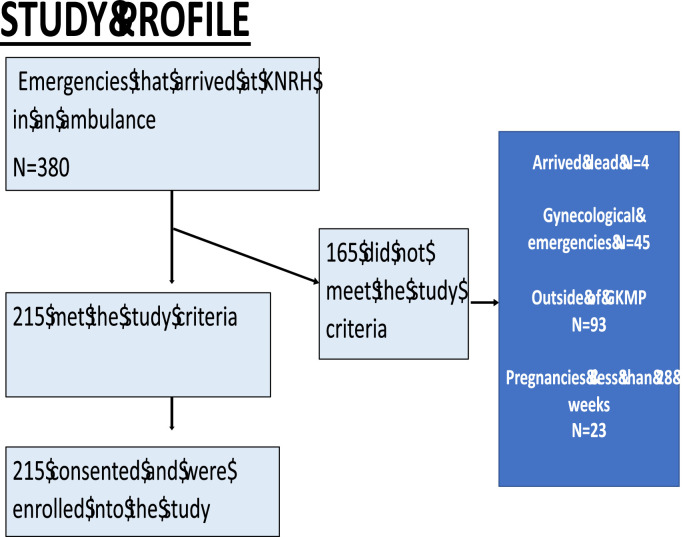
The study was based at KNRH in Kampala, Uganda. It was a descriptive and analytic cross-sectional study. Trained research assistants enrolled participating patients who met the inclusion criteria consecutively on arrival by ambulance at the hospital. Utilizing a questionnaire, quantitative data was collected from the ambulance driver, the sending facility referral form, and the receiving hospital's ambulance log book for each case. The sample size was 215.
Results
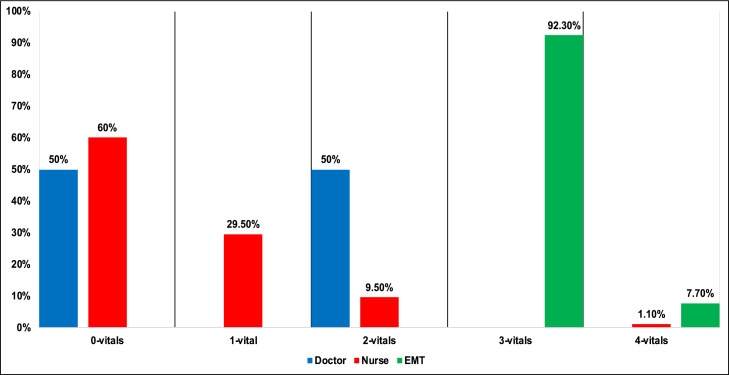
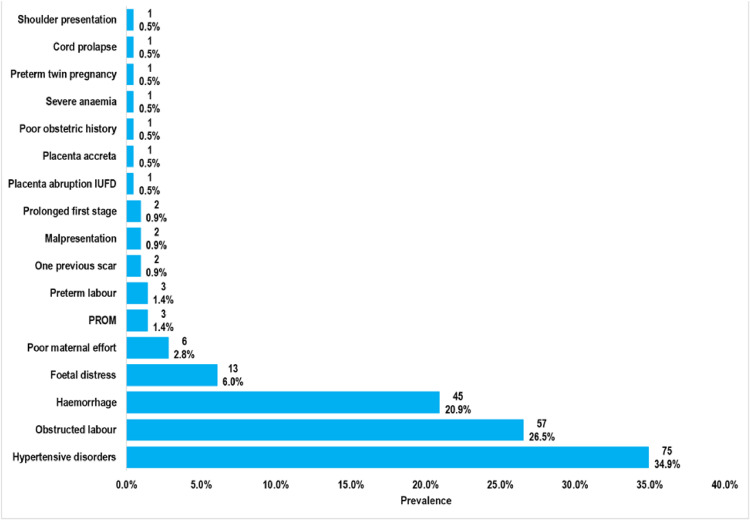
The median age was 27 years and the majority of patients were referred because of hypertensive disorders (34.9%), obstructed labor (26.5%) and hemorrhage (20.9%). The median total response time for transfer of obstetric emergencies was 50 min, from ambulance activation until the mother was received at KNRH. Differences were identified between government and non-government-owned ambulances in regards to the method of activation, medical escort staffing, number of vital signs recorded, and ambulance onboard medical care. Ambulances parked at the facility took the shortest transfer time and EMT-supported ambulances had the greatest number of vital signs taken.
Conclusions
Recommendations are to develop an integrated ambulance system for both government and non-government ambulances with standards especially in regards to standardized scripted call-center calls analysis, dispatch activation time, response-to-patient time, and trained ambulance professional staffing and medical care whenever in patient transport mode.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
